

The Effectiveness of Transcranial Brain Stimulation in Improving Clinical Signs of Hyperkinetic Movement Disorders
- PMID: 26778947
- PMCID: PMC4703824
- DOI: 10.3389/fnins.2015.00486
The Effectiveness of Transcranial Brain Stimulation in Improving Clinical Signs of Hyperkinetic Movement Disorders
Abstract
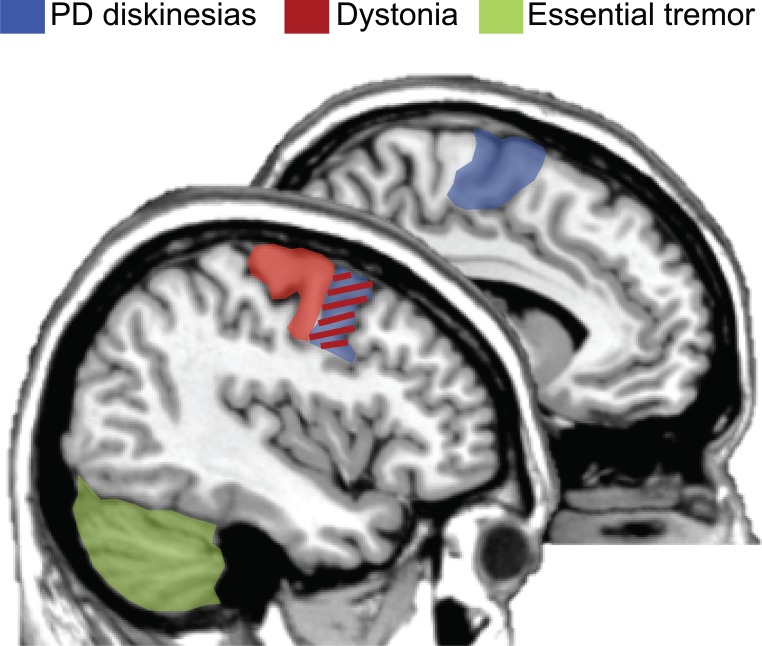
Repetitive transcranial magnetic stimulation (rTMS) is a safe and painless method for stimulating cortical neurons. In neurological realm, rTMS has prevalently been applied to understand pathophysiological mechanisms underlying movement disorders. However, this tool has also the potential to be translated into a clinically applicable therapeutic use. Several available studies supported this hypothesis, but differences in protocols, clinical enrollment, and variability of rTMS effects across individuals complicate better understanding of efficient clinical protocols. The aim of this present review is to discuss to what extent the evidence provided by the therapeutic use of rTMS may be generalized. In particular, we attempted to define optimal cortical regions and stimulation protocols that have been demonstrated to maximize the effectiveness seen in the actual literature for the three most prevalent hyperkinetic movement disorders: Parkinson's disease (PD) with levodopa-induced dyskinesias (LIDs), essential tremor (ET) and dystonia. A total of 28 rTMS studies met our search criteria. Despite clinical and methodological differences, overall these studies demonstrated that therapeutic applications of rTMS to "normalize" pathologically decreased or increased levels of cortical activity have given moderate progress in patient's quality of life. Moreover, the present literature suggests that altered pathophysiology in hyperkinetic movement disorders establishes motor, premotor or cerebellar structures as candidate regions to reset cortico-subcortical pathways back to normal. Although rTMS has the potential to become a powerful tool for ameliorating the clinical outcome of hyperkinetic neurological patients, until now there is not a clear consensus on optimal protocols for these motor disorders. Well-controlled multicenter randomized clinical trials with high numbers of patients are urgently required.
Keywords: Parkinson's disease; dystonia; essential tremor; levodopa-induced dyskinesias; rTMS.
Figures
References
-
- Allam N., Brasil-Neto J. P., Brandão P., Weiler F., Barros Filho J. d., Tomaz C. (2007). Relief of primary cervical dystonia symptoms by low frequency transcranial magnetic stimulation of the premotor cortex: case report. Arq. Neuropsiquiatr. 65, 697–699. 10.1590/S0004-282X2007000400030 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous