

Dermatofibrosarcoma protuberans: from translocation to targeted therapy
- PMID: 26779374
- PMCID: PMC4706526
- DOI: 10.7497/j.issn.2095-3941.2015.0067
Dermatofibrosarcoma protuberans: from translocation to targeted therapy
Abstract
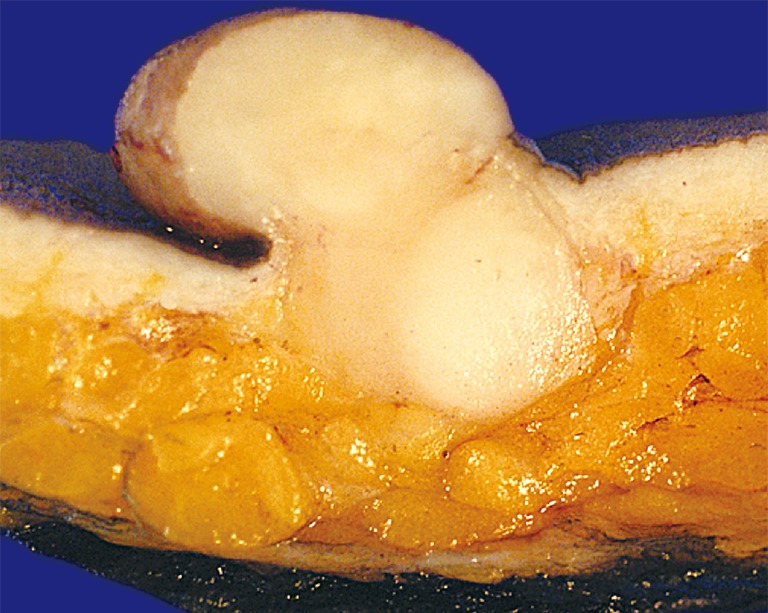
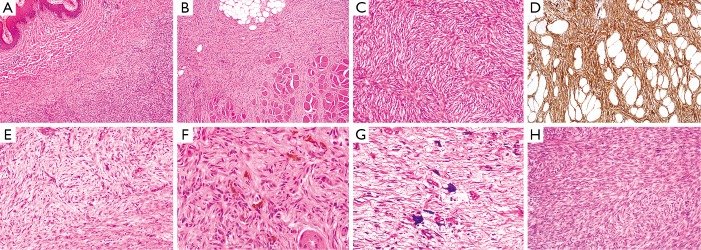
Dermatofibrosarcoma protuberans (DFSP), the most common dermal sarcoma, is a low-grade, slow growing fibroblastic malignant neoplasm that most frequently affects middle aged adults and is characterized by a high local recurrence rate and a low propensity for metastasis. Wide surgical resection or Mohs micrographic surgery (MMS) are the preferred approaches for localized disease, while radiation therapy is warranted for inoperable disease or for cases with positive margins where re-excision is not possible. DFSP is generally regarded as refractory to conventional chemotherapy. Treatment options for systemic disease were limited until the discovery of a unique translocation, t(17;22)(q22;q13) (COL1A1;PDGFB) found in a majority of cases. In recent years, imatinib, a PDGFβR, ABL and KIT inhibitor, has revolutionized systemic therapy in DFSP. In this review, we summarize the epidemiological, clinical, histological and genetic characteristics of DFSP and update the readers on its current management.
Keywords: Dermatofibrosarcoma protuberans (DFSP); Mohs micrographic surgery (MMS); imatinib; targeted therapy; translocation.
Conflict of interest statement
No potential conflicts of interest are disclosed.
Figures
References
-
- Fletcher CDM BJ, Hogendoorn PCW, Mertens F. WHO Classification of Tumours of Soft Tissue and Bone. Pathology and Genetics of Tumours of Soft Tissue and Bone. IARC Press 2013.
-
- Criscione VD, Weinstock MA. Descriptive epidemiology of dermatofibrosarcoma protuberans in the United States, 1973 to 2002. J Am Acad Dermatol 2007;56:968-973. - PubMed
-
- Bowne WB, Antonescu CR, Leung DH, Katz SC, Hawkins WG, Woodruff JM, et al. Dermatofibrosarcoma protuberans: A clinicopathologic analysis of patients treated and followed at a single institution. Cancer 2000;88:2711-2720. - PubMed
-
- Rutgers EJ, Kroon BB, Albus Lutter CE, Gortzak E. Dermatofibrosarcoma protuberans: treatment and prognosis. Eur J Surg Oncol 1992;18:241-248. - PubMed
-
- Valdivielso-Ramos M, Hernanz JM. Dermatofibrosarcoma protuberans in childhood. Actas Dermosifiliogr 2012;103:863-873. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous