

The Copenhagen City Heart Study (Østerbroundersøgelsen)
- PMID: 26779513
- PMCID: PMC4625209
- DOI: 10.5339/gcsp.2015.33
The Copenhagen City Heart Study (Østerbroundersøgelsen)
Abstract
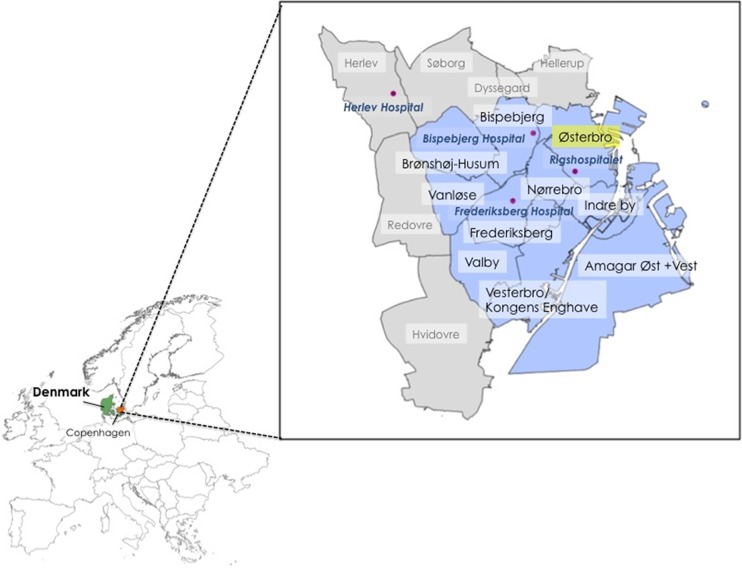
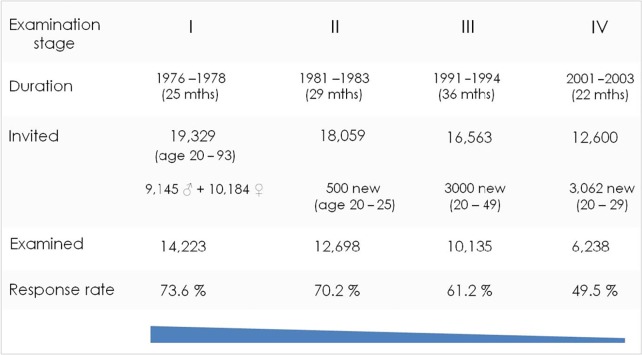
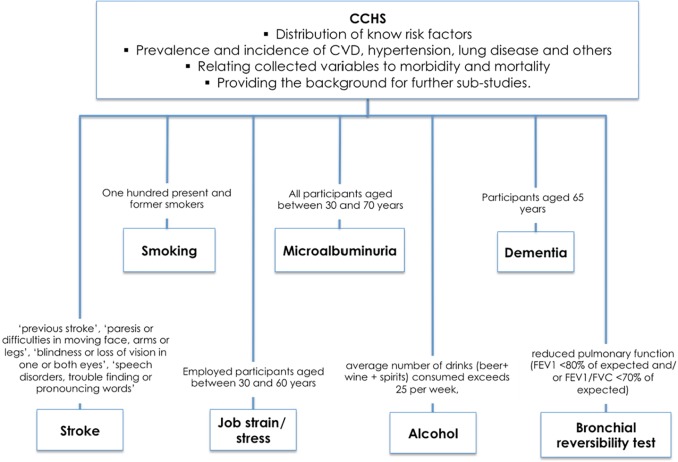
The Copenhagen City Heart Study, also known as "Østerbroundersøgelsen", is a large prospective cardio-vascular population study of 20,000 women and men that was launched in 1975 by Dr Peter Schnohr and Dr Gorm Jensen together with statistician Jørgen Nyboe and Prof. A. Tybjærg Hansen. The original purpose of the study was to focus on prevention of coronary heart disease and stroke. During the years many other aspects have been added to the study: pulmonary diseases, heart failure, arrhythmia, alcohol, arthrosis, eye diseases, allergy, epilepsia, dementia, stress, vital exhaustion, social network, sleep-apnoe, ageing and genetics. In this review we highlight unique aspects of the Copenhagen City Heat Study (CCHS) and its outcome in investigations of clinical and molecular aspects of health and disease in the regional and global population. To increase the impact of population studies with a focus on risk and prevention of cardiovascular and related diseases and to maximize the likelihood of identifying disease causes and effective therapeutics, lessons learned from past research should be applied to the design, implementation and interpretation of future studies.
Figures

References
-
- Epidemiology of chest pain and angina pectoris, with special reference to treatment needs Jensen G, ed. Acta Med Scand; suppl 682 Thesis; 1984. - PubMed
-
- Appleyard M, Hansen AT, Schnohr P, Jensen G, Nyboe J, The Copenhagen City Heart Study Øster- broundersøgelsen. A book of tables with data from the first examination (1976–78) and a five year follow-up (1981–83) Scand J Soc Med. 1989;170(suppl 41):1–160. - PubMed
-
- Schnohr P, Jensen G, Lange P, Scharling H, Appleyard M. Tables with data from the third examination 1991–94. Eur Heart J. 2001;3(suppl H)
-
- Schnohr P. Physical activity in leisure time: impact on mortality. Risks and benefits. Dan Med Bull. 2009;56(1):40–71. Review. - PubMed
-
- Rose GA, Blackburn H. Cardiovascular survey methods. Geneva: Wld Health Org Monogr Ser 56 1968; - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous