

PCSK9 inhibitors and cardiovascular disease: heralding a new therapeutic era
- PMID: 26780005
- PMCID: PMC4927326
- DOI: 10.1097/MOL.0000000000000239
PCSK9 inhibitors and cardiovascular disease: heralding a new therapeutic era
Abstract
Purpose of review: The first monoclonal antibodies targeting proprotein convertase subtilisin/kexin type 9 (PCSK9) have been approved for clinical use. This timely review highlights recent developments.
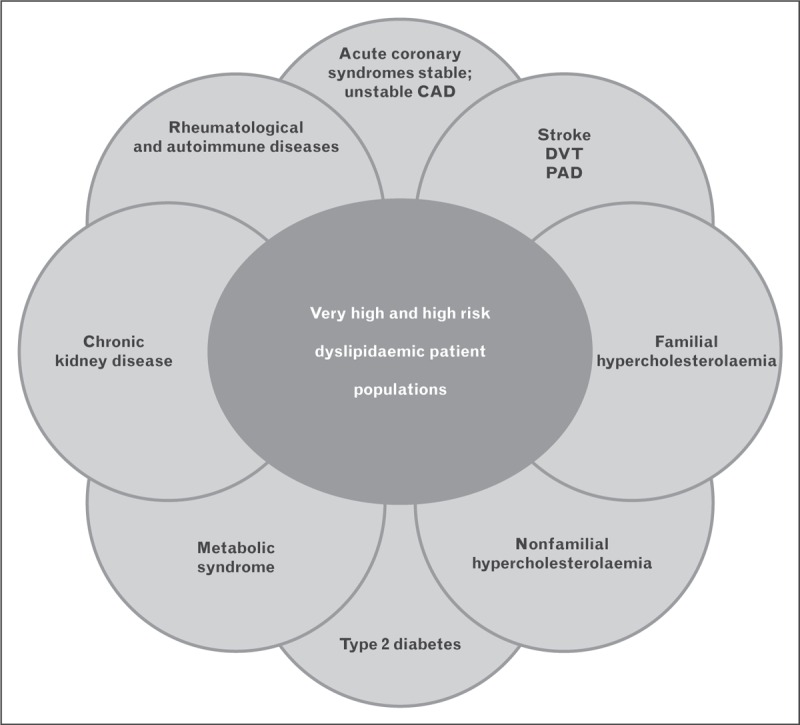
Recent findings: Low-density lipoprotein cholesterol (LDL-C) is the primary driver of atherosclerosis and the key target for intervention. Yet despite best treatment including statins, attaining sufficient LDL-C lowering can be problematic for high cardiovascular risk patients. The development of PCSK9 inhibitors, driven by novel genetic and mechanistic insights, offers an answer. Removal of circulating PCSK9 increases LDL receptor availability, and thus markedly decreases plasma LDL-C levels (by ∼50-60%), and is additive to the lipid lowering effects of statins and ezetimibe. PCSK9 inhibition also reduces (by 25-30%) plasma levels of lipoprotein(a), a causal factor in atherosclerotic vascular disease, suggestive of partial catabolism of lipoprotein(a) by LDL receptors. The ODYSSEY and PROFICIO (Programme to Reduce LDL-C and Cardiovascular Outcomes Following Inhibition of PCSK9 In Different Populations) clinical trial programmes involving a wide range of high-risk patients, including statin intolerant patients, have confirmed the consistency of the LDL response, even with concomitant high-intensity statin or nonstatin therapy. Extensive evidence to date attests to a favourable safety and tolerability profile for these innovative agents.
Summary: The new pharmacotherapeutic era of PCSK9 inhibition is upon us, promising major reduction in cardiovascular events across a wide spectrum of high-risk patients.
Figures


References
-
- World Health Organization. Top 10 causes of death. http://www.who.int/mediacentre/factsheets/fs310/en/index2.html [Accessed 18 August 2015]
-
- World Economic Forum and Harvard School of Public Health. The global economic burden of Noncommunicable Diseases. 2011. http://www3.weforum.org/docs/WEF_Harvard_HE_GlobalEconomicBurdenNonCommu... [Accessed 3 September 2015]
-
- Ference BA, Majeed F, Penumetcha R, et al. Effect of naturally random allocation to lower low-density lipoprotein cholesterol on the risk of coronary heart disease mediated by polymorphisms in NPC1L1, HMGCR, or both: a 2 × 2 factorial Mendelian randomization study. J Am Coll Cardiol 2015; 65:1552–1561. - PMC - PubMed
-
The outstanding study provides unique insights into facets of genetically determined CHD risk using a Mendelian randomization approach.
-
- Reiner Z, Catapano AL, De Backer G, et al. ESC/EAS Guidelines for the management of dyslipidaemias: the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Eur Heart J 2011; 32:1769–1818. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
