

Distinctive Electrocardiographic Features in African Americans Diagnosed with Takotsubo Cardiomyopathy
- PMID: 26780323
- PMCID: PMC6931853
- DOI: 10.1111/anec.12337
Distinctive Electrocardiographic Features in African Americans Diagnosed with Takotsubo Cardiomyopathy
Abstract
Background: Takotsubo cardiomyopathy (TC) can resemble acute anterior ST-elevation myocardial infarction. Most studies have examined TC in Asians and Caucasians (non-African Americans [AA]), while very few cases have been reported in AA. We aimed to assess the electrocardiographic features of TC in AA patients and compare them to non-AA TC patients.
Methods: We retrospectively compared electrocardiograms of 52 AA and 47 non-AA patients diagnosed with TC. All patients met the modified Mayo Clinic criteria for the diagnosis of TC. Information collected included PR interval, QRS duration and amplitude, QT interval in milliseconds (msec) adjusted for heart rate (QTc), ST-segment deviation at the J point in limb and precordial leads (≥1 mm), ST elevation (≥1 mm), and T-wave inversion (≥0.5 mm).
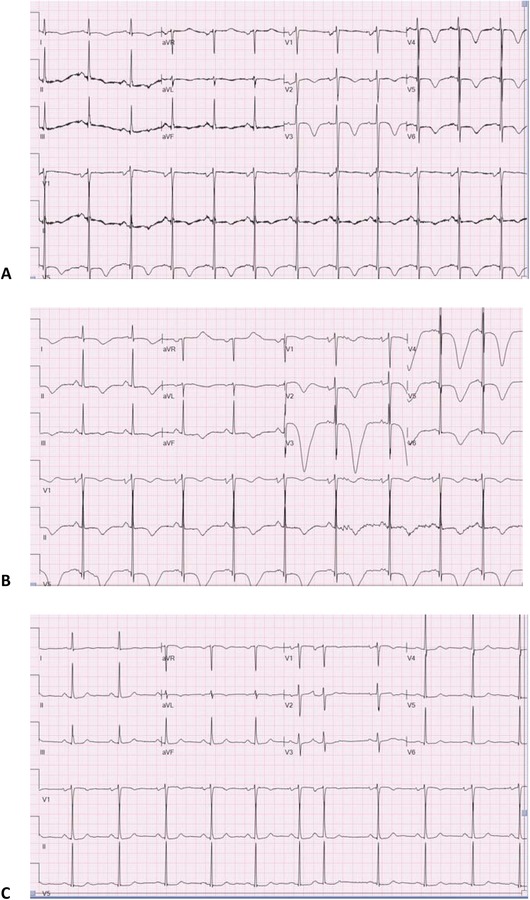
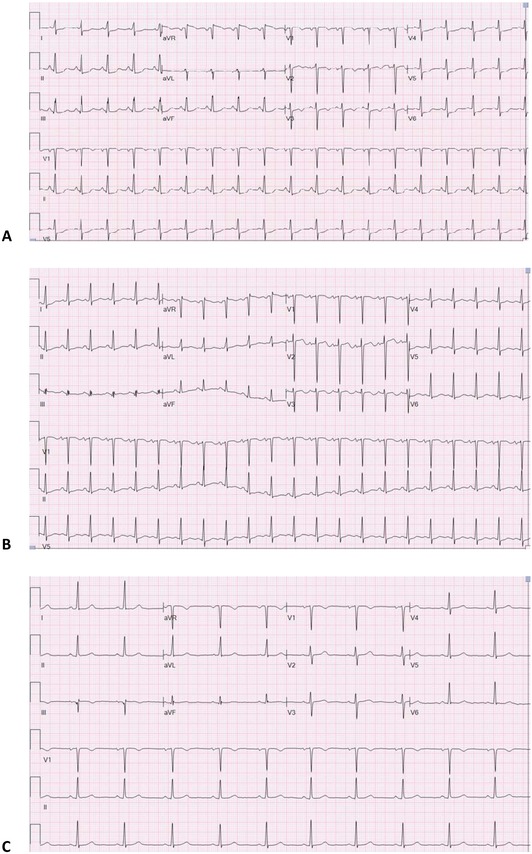
Results: T-wave inversion was more prevalent on presentation among AA patients (82% vs 48% in non-AA; P < 0.01), whereas ST depression was more common among non-AA (21% vs 7% in AA; P = 0.05). T-wave inversions in AA patients were frequent in both limb and precordial leads, whereas T-wave inversions in non-AA were limited to precordial leads. The average QTc upon presentation in AA was longer than non-AA (491 msec in AA vs 456 msec in non-AA; P < 0.01) as was the maximum average QTc during index hospitalization (527 msec in AA vs 497 msec in non-AA, P = 0.03).
Conclusion: In patients presenting with TC, AA patients more frequently present with diffuse T-wave inversions and a more prolonged QTc, whereas non-AA patients more often present with ST depressions. AA patients also more frequently present with T-wave inversions diffusely, whereas non-AA patients present with T-wave inversions more limited to the precordial leads.
Keywords: African American; apical ballooning; cardiomyopathy; electrocardiography; takotsubo.
© 2016 Wiley Periodicals, Inc.
Figures
Comment in
-
Electrocardiograms in African Americans and Non-African Americans Presenting with Takotsubo Syndrome.Ann Noninvasive Electrocardiol. 2017 Jan;22(1):e12381. doi: 10.1111/anec.12381. Epub 2016 Jun 2. Ann Noninvasive Electrocardiol. 2017. PMID: 27251743 Free PMC article. No abstract available.
-
Racial and Ethnic Differences in Electrocardiographic Features of Takotsubo Cardiomyopathy.Ann Noninvasive Electrocardiol. 2017 Jan;22(1):e12380. doi: 10.1111/anec.12380. Epub 2016 Jun 2. Ann Noninvasive Electrocardiol. 2017. PMID: 27253398 Free PMC article. No abstract available.
References
-
- Gianni M, Dentali F, Grandi AM, et al. Apical ballooning syndrome or takotsubo cardiomyopathy: A systematic review. Eur Heart J 2006;27:1523–1529. - PubMed
-
- Perazzolo M, Zorzi A, Orbetti F, et al. Apicobasal gradient of left ventricular myocardial edema underlies transient T‐wave inversion and QT interval prolongation (Wellens' ECG pattern) in Tako‐Tsubo cardiomyopathy. Heart Rhythm 2013;10:70–77. - PubMed
-
- Kurisu S, Inoue I, Kawagoe T, et al. Time course of electrocardiographic changes in patients with tako‐tsubo syndrome: Comparison with acute myocardial infarction with minimal enzymatic release. Circ J 2004;68:77–81. - PubMed
-
- Parkkonen O, Allonen J, Vaara S, et al. Differences in ST‐elevation and T‐wave amplitudes do not reliably differentiate takotsubo cardiomyopathy from acute anterior myocardial infarction. J Electrocardiol 2014;47:692–699. - PubMed
-
- Dib C, Asirvatham S, Elesber A, et al. Clinical correlates and prognostic significance of electrocardiographic abnormalities in apical ballooning syndrome (Takotsubo/stress‐induced cardiomyopathy). Am Heart J 2009;157(5):933–938. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
