

A technique for pediatric chest wall reconstruction using custom-designed titanium implants: description of technique and report of two cases
- PMID: 26782367
- PMCID: PMC4763153
- DOI: 10.1007/s11832-015-0709-1
A technique for pediatric chest wall reconstruction using custom-designed titanium implants: description of technique and report of two cases
Abstract
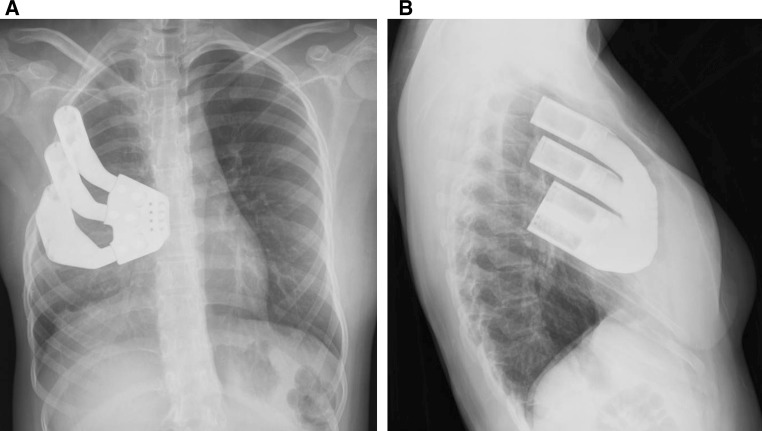
Purpose: We present a surgical technique for chest wall reconstruction using custom-designed titanium implants developed for two female patients to provide both chest wall symmetry and adequate stability for staged breast reconstruction.
Methods: A retrospective review was performed for two adolescent female patients with large chest wall defects who underwent the described technique. The etiology of the chest wall deficiency was secondary to Poland's syndrome in one patient, and secondary to surgical resection of osteosarcoma in the other patient. For each patient, a fine-cut computed tomography scan was obtained to assist with implant design. After fabrication of the prosthesis, reconstruction was performed though a curvilinear thoracotomy approach with attachment of the implant to the adjacent ribs and sternum. Wound closure was obtained with use of synthetic graft material, local soft tissue procedures, and flap procedures as necessary.
Results: The two patients were followed post-operatively for 35 and 38 months, respectively. No intra-operative or post-operative complications were identified. Mild scoliosis that had developed in the patient following chest wall resection for osteosarcoma did not demonstrate any further progression following reconstruction.
Conclusions: We conclude that this technique was successful at providing a stable chest wall reconstruction with satisfactory cosmetic results in our patients.
Keywords: Chest wall deficiency; Chest wall reconstruction; Chest wall resection; Pediatric orthopedics; Poland’s syndrome.
Figures






References
LinkOut - more resources
Full Text Sources
Other Literature Sources
