

Treatment of Intravenous Leiomyomatosis with Cardiac Extension following Incomplete Resection
- PMID: 26783463
- PMCID: PMC4689968
- DOI: 10.1155/2015/756141
Treatment of Intravenous Leiomyomatosis with Cardiac Extension following Incomplete Resection
Abstract
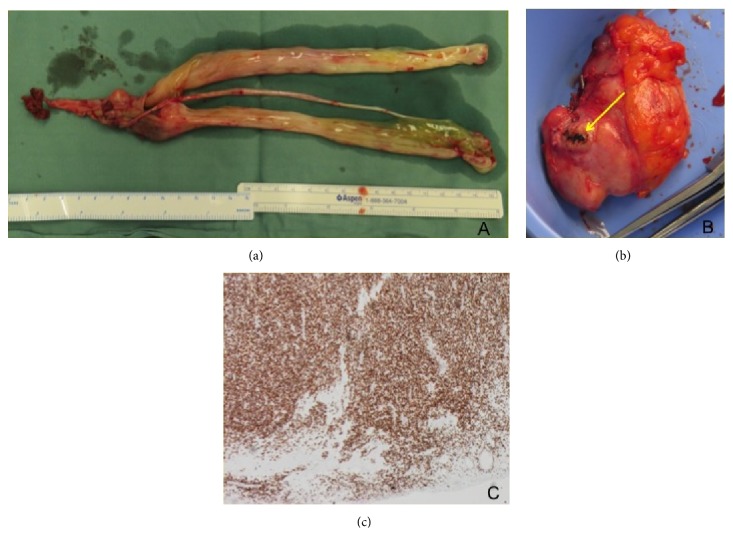
Aim. Intravenous leiomyomatosis (IVL) with cardiac extension (CE) is a rare variant of benign uterine leiomyoma. Incomplete resection has a recurrence rate of over 30%. Different hormonal treatments have been described following incomplete resection; however no standard therapy currently exists. We review the literature for medical treatments options following incomplete resection of IVL with CE. Methods. Electronic databases were searched for all studies reporting IVL with CE. These studies were then searched for reports of patients with inoperable or incomplete resection and any further medical treatments. Our database was searched for patients with medical therapy following incomplete resection of IVL with CE and their results were included. Results. All studies were either case reports or case series. Five literature reviews confirm that surgery is the only treatment to achieve cure. The uses of progesterone, estrogen modulation, gonadotropin-releasing hormone antagonism, and aromatase inhibition have been described following incomplete resection. Currently no studies have reviewed the outcomes of these treatments. Conclusions. Complete surgical resection is the only means of cure for IVL with CE, while multiple hormonal therapies have been used with varying results following incomplete resection. Aromatase inhibitors are the only reported treatment to prevent tumor progression or recurrence in patients with incompletely resected IVL with CE.
Figures
Similar articles
-
Update on intravenous leiomyomatosis: report of five patients and literature review.Eur J Obstet Gynecol Reprod Biol. 2013 Dec;171(2):209-13. doi: 10.1016/j.ejogrb.2013.09.031. Epub 2013 Oct 5. Eur J Obstet Gynecol Reprod Biol. 2013. PMID: 24207051 Review.
-
Intravenous leiomyomatosis treated with radical hysterectomy and adjuvant aromatase inhibitor therapy.J Obstet Gynaecol Res. 2016 Oct;42(10):1405-1408. doi: 10.1111/jog.13063. Epub 2016 Jul 19. J Obstet Gynaecol Res. 2016. PMID: 27436168
-
Management and prognosis comparison between incidental and nonincidental intravenous leiomyomatosis: a retrospective single-center real-life experience.Ann Transl Med. 2022 May;10(9):503. doi: 10.21037/atm-21-5376. Ann Transl Med. 2022. PMID: 35692495 Free PMC article.
-
Massive pelvic recurrence of uterine leiomyomatosis with intracaval-intracardiac extension: video case report and literature review.BMC Surg. 2017 Nov 29;17(1):118. doi: 10.1186/s12893-017-0306-y. BMC Surg. 2017. PMID: 29187188 Free PMC article. Review.
-
Pathological characteristics and clinical prognostic analysis of intravenous leiomyomatosis: a retrospective study of 43 cases.Front Med (Lausanne). 2025 Apr 10;12:1534933. doi: 10.3389/fmed.2025.1534933. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40276735 Free PMC article.
Cited by
-
The optimal diagnosis and treatment of intravenous leimyomatosis.Cardiovasc J Afr. 2023 Jan-Apr 23;34(1):44-47. doi: 10.5830/CVJA-2022-002. Epub 2022 Jul 4. Cardiovasc J Afr. 2023. PMID: 35789358 Free PMC article.
-
Different surgical strategies of patients with intravenous leiomyomatosis.Medicine (Baltimore). 2016 Sep;95(37):e4902. doi: 10.1097/MD.0000000000004902. Medicine (Baltimore). 2016. PMID: 27631266 Free PMC article.
-
Uterineintravenous leiomyomatosis with cardiac involvement.Radiol Case Rep. 2020 Jun 28;15(8):1389-1393. doi: 10.1016/j.radcr.2020.05.053. eCollection 2020 Aug. Radiol Case Rep. 2020. PMID: 32636980 Free PMC article.
-
Post-hysterectomy intravenous leiomyomatosis: A case of successful multidisciplinary surgery under non-extracorporeal circulation.Mol Clin Oncol. 2017 Jan;6(1):39-43. doi: 10.3892/mco.2016.1074. Epub 2016 Nov 8. Mol Clin Oncol. 2017. PMID: 28123726 Free PMC article.
-
Intravenous Leiomyomatosis of the Uterus Extending to the Right Atrium: A Case Report.Ann Vasc Dis. 2025;18(1):24-00084. doi: 10.3400/avd.cr.24-00084. Epub 2025 Jan 21. Ann Vasc Dis. 2025. PMID: 39877328 Free PMC article.
References
-
- Ip P. P. C., Tse K. Y., Tam K. F. Uterine smooth muscle tumors other than the ordinary leiomyomas and leiomyosarcomas: a review of selected variants with emphasis on recent advances and unusual morphology that may cause concern for malignancy. Advances in Anatomic Pathology. 2010;17(2):91–112. doi: 10.1097/pap.0b013e3181cfb901. - DOI - PubMed
-
- Jung Choi I., Han M. S., Cha M. S. A huge case of intravenous leiomyomatosis with intracradiac extension. Journal of Womens Medicine. 2010;3(1):29–31.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
