

Improved Accuracy of Continuous Glucose Monitoring Systems in Pediatric Patients with Diabetes Mellitus: Results from Two Studies
- PMID: 26784126
- PMCID: PMC4717517
- DOI: 10.1089/dia.2015.0380
Improved Accuracy of Continuous Glucose Monitoring Systems in Pediatric Patients with Diabetes Mellitus: Results from Two Studies
Abstract
Objective: This study was designed to evaluate accuracy, performance, and safety of the Dexcom (San Diego, CA) G4(®) Platinum continuous glucose monitoring (CGM) system (G4P) compared with the Dexcom G4 Platinum with Software 505 algorithm (SW505) when used as adjunctive management to blood glucose (BG) monitoring over a 7-day period in youth, 2-17 years of age, with diabetes.
Research design and methods: Youth wore either one or two sensors placed on the abdomen or upper buttocks for 7 days, calibrating the device twice daily with a uniform BG meter. Participants had one in-clinic session on Day 1, 4, or 7, during which fingerstick BG measurements (self-monitoring of blood glucose [SMBG]) were obtained every 30 ± 5 min for comparison with CGM, and in youth 6-17 years of age, reference YSI glucose measurements were obtained from arterialized venous blood collected every 15 ± 5 min for comparison with CGM. The sensor was removed by the participant/family after 7 days.
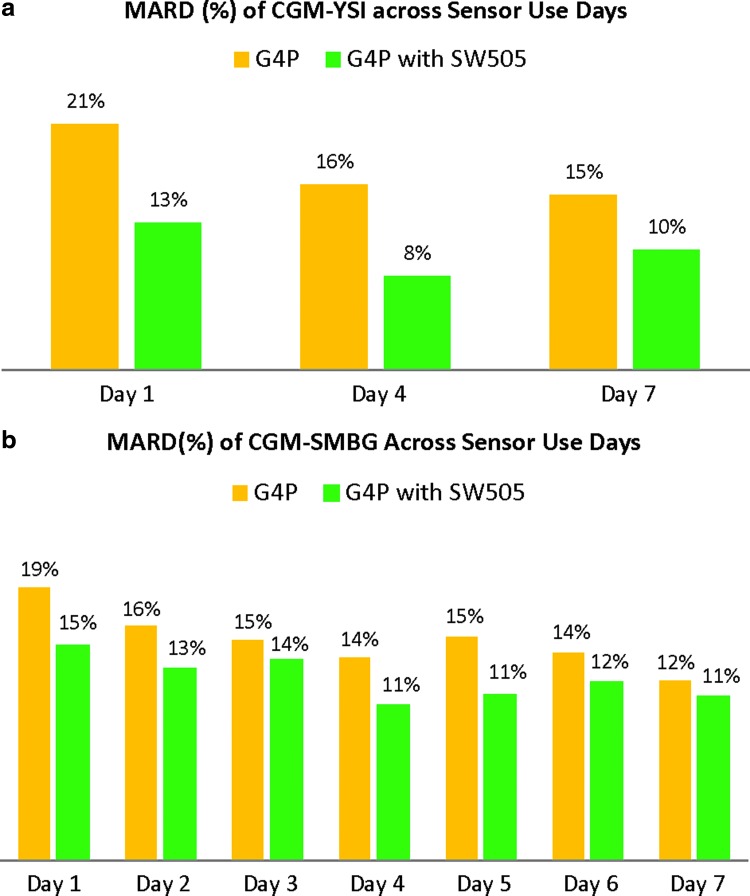
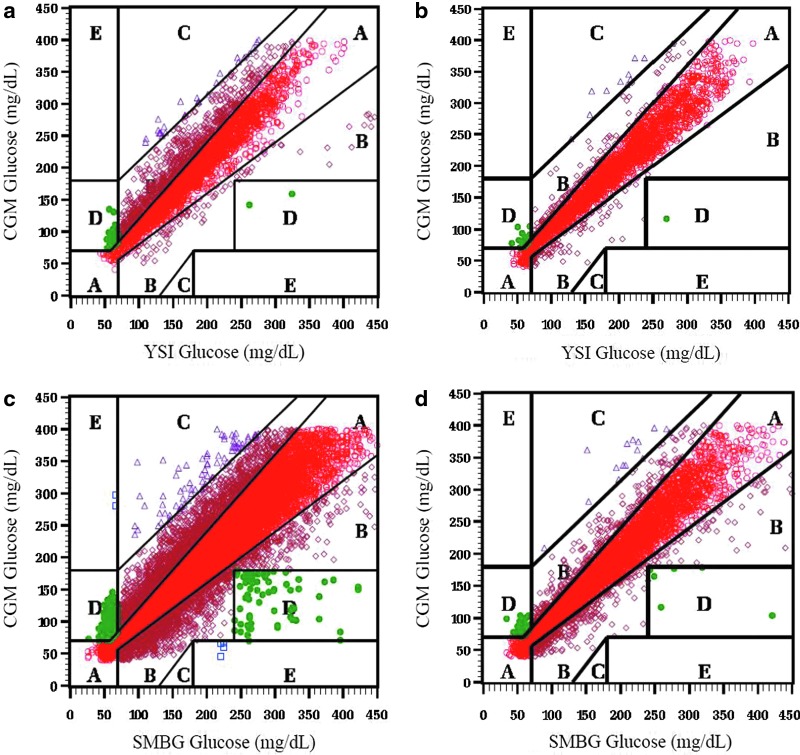
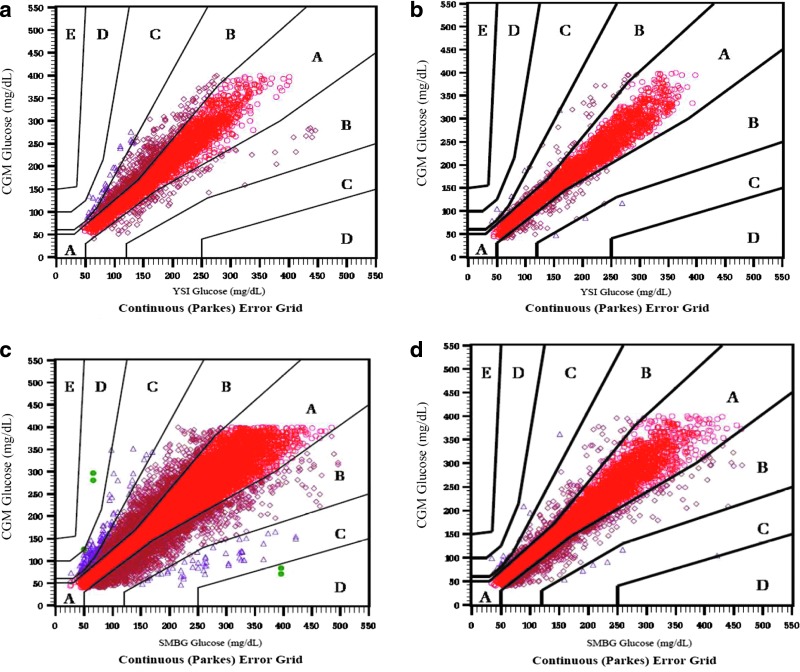
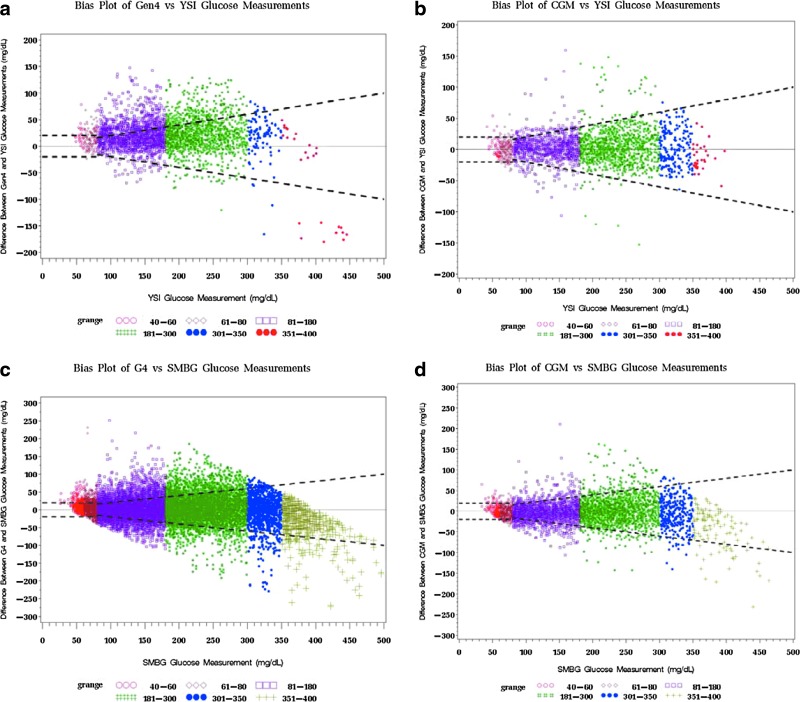
Results: In comparison of 2,922 temporally paired points of CGM with the reference YSI measurement for G4P and 2,262 paired points for SW505, the mean absolute relative difference (MARD) was 17% for G4P versus 10% for SW505 (P < 0.0001). In comparison of 16,318 temporally paired points of CGM with SMBG for G4P and 4,264 paired points for SW505, MARD was 15% for G4P versus 13% for SW505 (P < 0.0001). Similarly, error grid analyses indicated superior performance with SW505 compared with G4P in comparison of CGM with YSI and CGM with SMBG results, with greater percentages of SW505 results falling within error grid Zone A or the combined Zones A plus B. There were no serious adverse events or device-related serious adverse events for either the G4P or the SW505, and there was no sensor breakoff.
Conclusions: The updated algorithm offers substantial improvements in accuracy and performance in pediatric patients with diabetes. Use of CGM with improved performance has potential to increase glucose time in range and improve glycemic outcomes for youth.
Figures
References
-
- Petitti DB, Klingensmith GJ, Andrews JS, Bell RA, Dabelea D, Imperatore G, Linder B, Loots B, Marcovina SM, Pihoker C, Rodriguez BL, Standiford DA, Waitzfelder B, Mayer-Davis EJ; SEARCH for Diabetes in Youth Study: Glycemic control in youth with diabetes: the SEARCH for Diabetes in Youth Study. J Pediatr 2009;155:668–672 - PMC - PubMed
-
- Beck RW, Tamborlane WV, Bergenstal RM, Miller KM, DuBose SN, Hall CA; T1D Exchange Clinic Network: The T1D Exchange clinic registry. J Clin Endocrinol Metab 2012;97:4383–4389 - PubMed
-
- Wood JR, Miller KM, Maahs DM, Beck RW, DiMeglio LA, Libman IM, Quinn M, Tamborlane WV, Woerner SE; T1D Exchange Clinic Network: Most youth with type 1 diabetes in the T1D Exchange Clinic Registry do not meet American Diabetes Association or International Society for Pediatric and Adolescent Diabetes clinical guidelines. Diabetes Care 2013;36:2035–2037 - PMC - PubMed
-
- Miller KM, Foster NC, Beck RW, Bergenstal RM, DuBose SN, DiMeglio LA, Maahs DM, Tamborlane WV; T1D Exchange Clinic Network: Current state of type 1 diabetes treatment in the U.S.: updated data from the T1D Exchange clinic registry. Diabetes Care 2015;38:971–978 - PubMed
-
- Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group: Continuous glucose monitoring and intensive treatment of type 1 diabetes. N Engl J Med 2008;359:1464–1476 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical