

Chronic Exposure to Androgenic-Anabolic Steroids Exacerbates Axonal Injury and Microgliosis in the CHIMERA Mouse Model of Repetitive Concussion
- PMID: 26784694
- PMCID: PMC4718534
- DOI: 10.1371/journal.pone.0146540
Chronic Exposure to Androgenic-Anabolic Steroids Exacerbates Axonal Injury and Microgliosis in the CHIMERA Mouse Model of Repetitive Concussion
Abstract
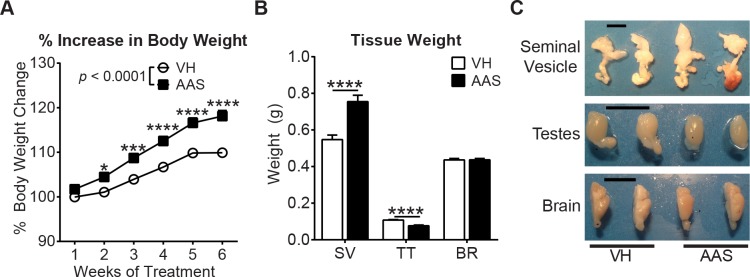
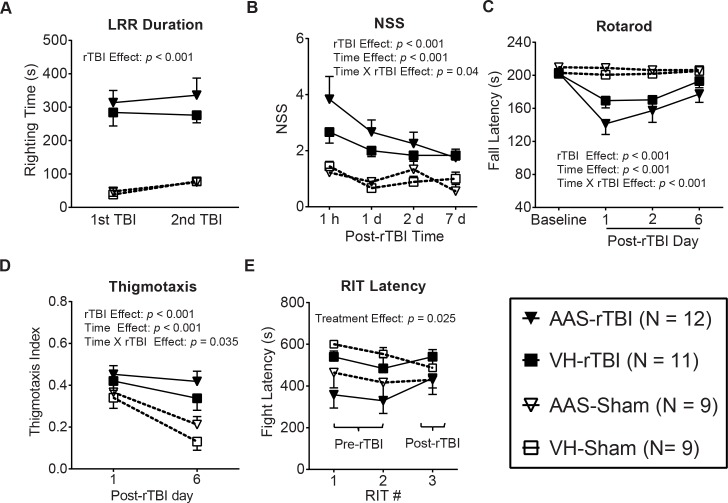
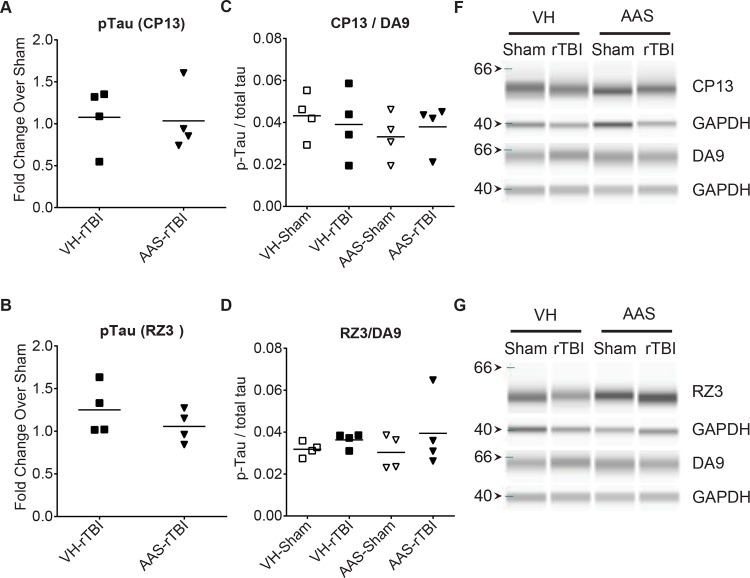
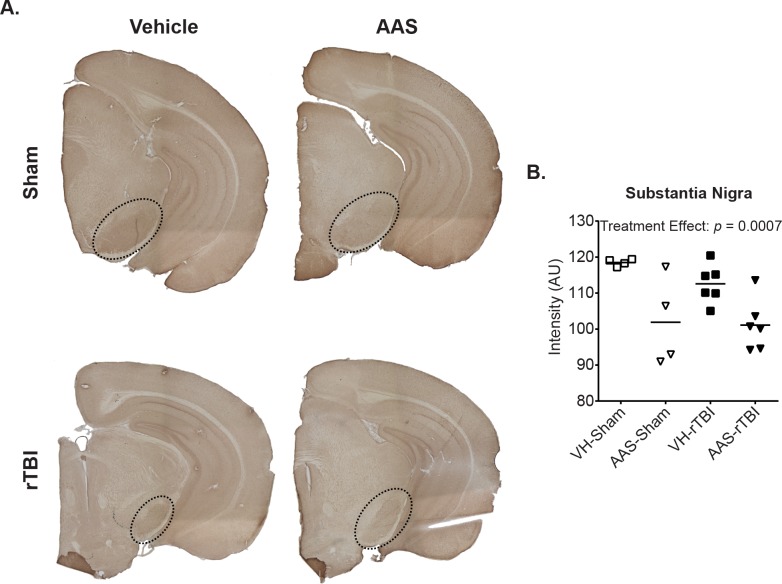
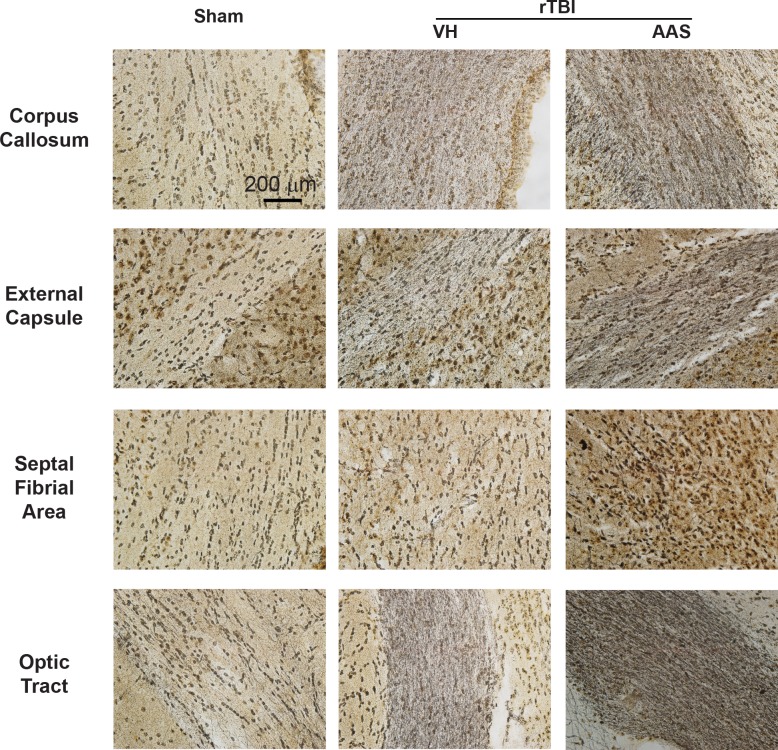
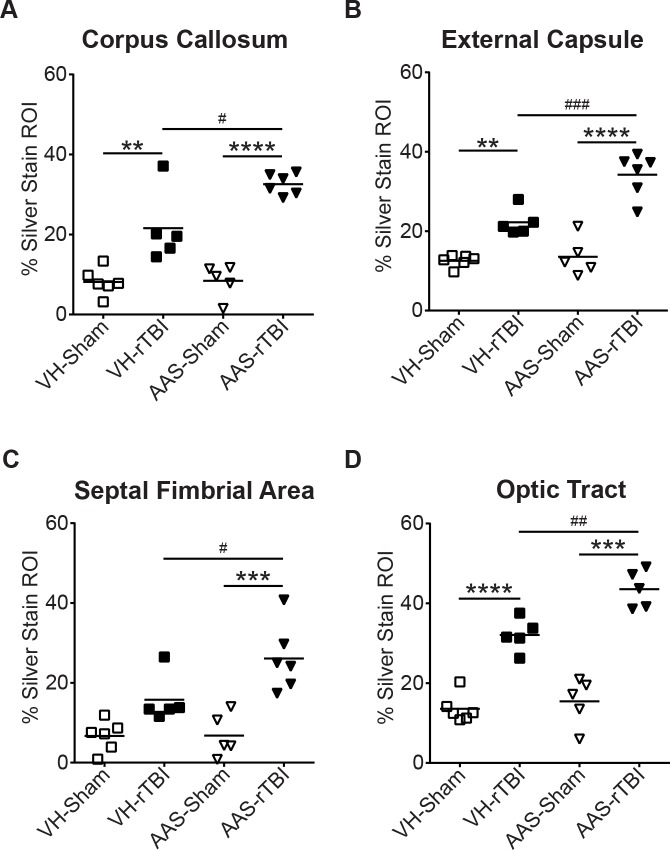
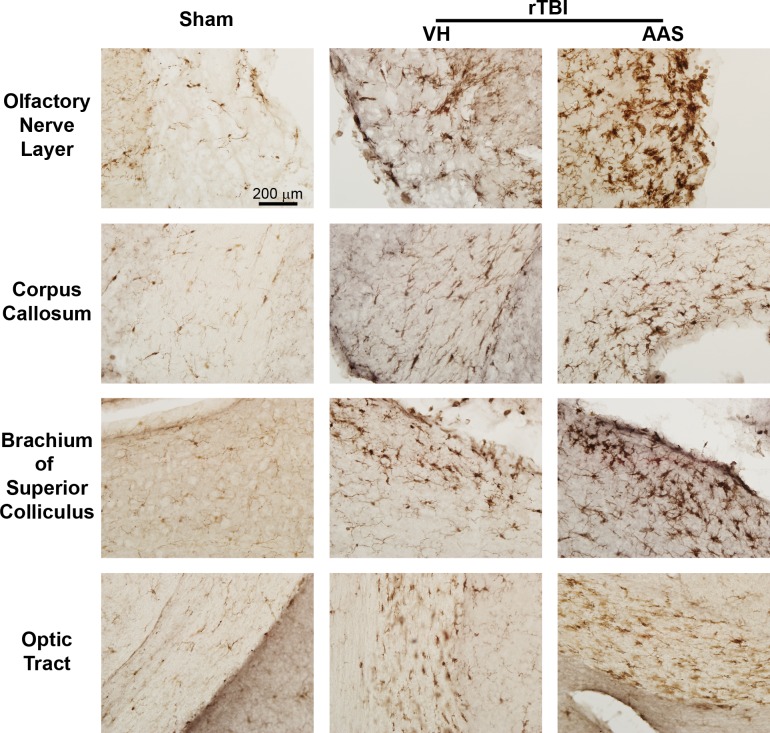
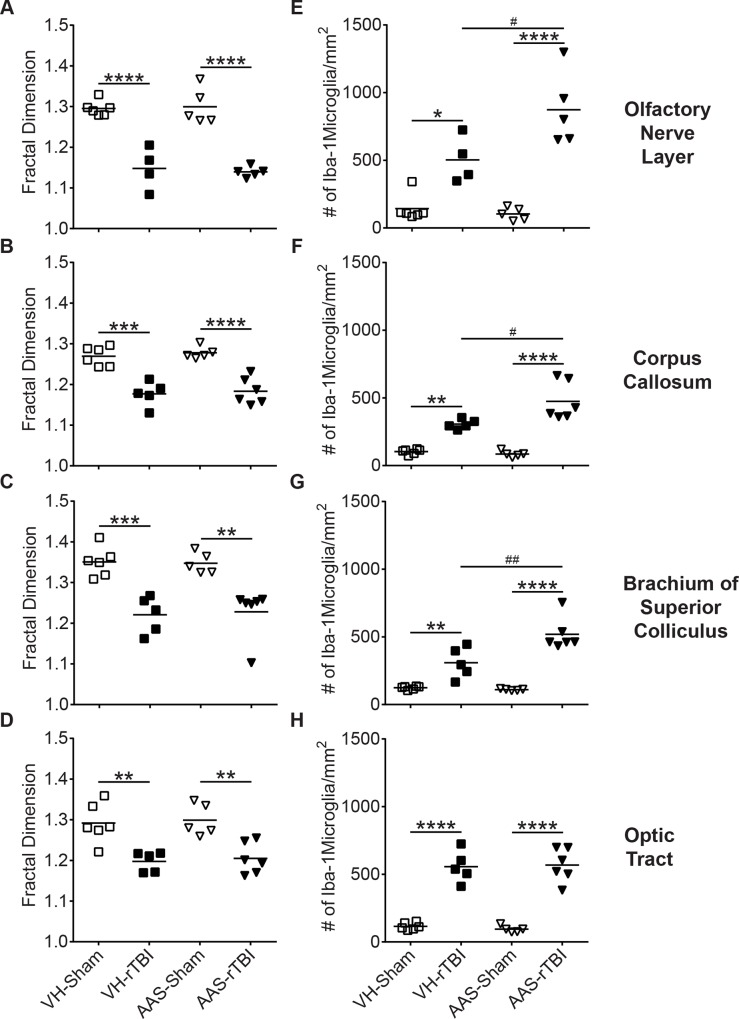
Concussion is a serious health concern. Concussion in athletes is of particular interest with respect to the relationship of concussion exposure to risk of chronic traumatic encephalopathy (CTE), a neurodegenerative condition associated with altered cognitive and psychiatric functions and profound tauopathy. However, much remains to be learned about factors other than cumulative exposure that could influence concussion pathogenesis. Approximately 20% of CTE cases report a history of substance use including androgenic-anabolic steroids (AAS). How acute, chronic, or historical AAS use may affect the vulnerability of the brain to concussion is unknown. We therefore tested whether antecedent AAS exposure in young, male C57Bl/6 mice affects acute behavioral and neuropathological responses to mild traumatic brain injury (TBI) induced with the CHIMERA (Closed Head Impact Model of Engineered Rotational Acceleration) platform. Male C57Bl/6 mice received either vehicle or a cocktail of three AAS (testosterone, nandrolone and 17α-methyltestosterone) from 8-16 weeks of age. At the end of the 7th week of treatment, mice underwent two closed-head TBI or sham procedures spaced 24 h apart using CHIMERA. Post-repetitive TBI (rTBI) behavior was assessed for 7 d followed by tissue collection. AAS treatment induced the expected physiological changes including increased body weight, testicular atrophy, aggression and downregulation of brain 5-HT1B receptor expression. rTBI induced behavioral deficits, widespread axonal injury and white matter microgliosis. While AAS treatment did not worsen post-rTBI behavioral changes, AAS-treated mice exhibited significantly exacerbated axonal injury and microgliosis, indicating that AAS exposure can alter neuronal and innate immune responses to concussive TBI.
Conflict of interest statement
Figures
References
-
- Gerberding JL, Binder S. The report to congress on mild traumatic brain injury in the United States: Steps to prevent a serious public health problem Atlanta, GA: Centers for Disease Control and Prevention, 2003.
-
- Langlois JA, Rutland-Brown W, Wald MM. The Epidemiology and Impact of Traumatic Brain Injury: A Brief Overview. J Head Trauma Rehabil. 2006;21(5):375–8. - PubMed
-
- Faul MM, Xu L, Wald MM, Coronado VG. Traumatic brain injury in the united states: emergency department visits, hospitalizations and death 2002–2006 Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, 2010.
-
- Centers for Disease Control and Prevention. Nonfatal traumatic brain injuries related to sports and recreation activities among persons aged <19 years—United States, 2001–2009. MMWR Morb Mortal Wkly Rep. 2011;30(39):1337–76. Epub 2007/07/28. doi: mm5629a2 [pii]. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
