

Cut-off values of latent infection in patients with rapid migration following bipolar hip hemiarthroplasty
- PMID: 26785746
- PMCID: PMC4719675
- DOI: 10.1186/s12891-016-0876-3
Cut-off values of latent infection in patients with rapid migration following bipolar hip hemiarthroplasty
Abstract
Background: Although most patients achieve favorable results following bipolar hip hemiarthroplasty (BHA), some experience rapid migration of the prosthesis. We retrospectively reviewed 18 patients with BHA that necessitated revision.
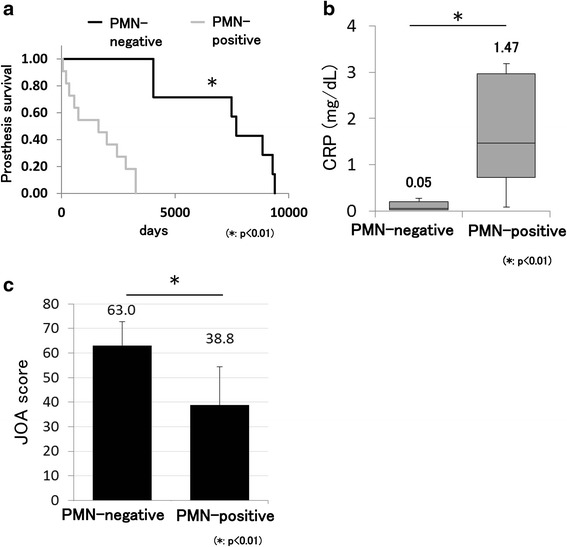
Methods: We examined soft tissues obtained from periprosthetic lesions. In total, 18 patients with pain and acetabular migration of the BHA prosthesis were included. The patients were divided into a polymorphonuclear leukocyte (PMN)-positive (≥5 PMNs per high-power field [HPF]) and PMN-negative (<5 PMNs/HPF) group.
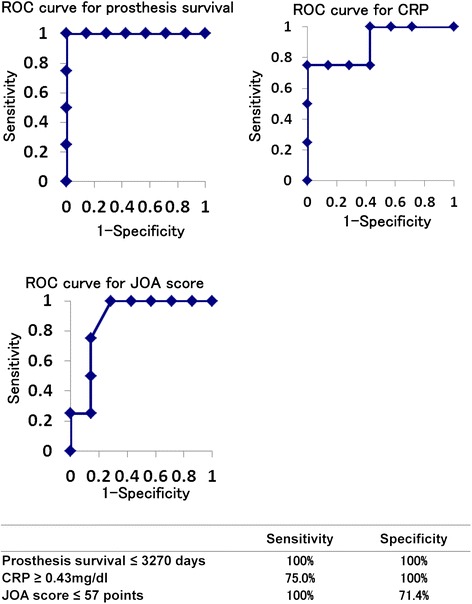
Results: Pathological findings showed that 11 patients were PMN-positive, which was indicative of infection. All patients in the PMN-positive group showed no polyethylene particles or foreign body giant cells, while all patients in the PMN-negative group showed polyethylene debris or foreign body giant cells (p < 0.001). BHA survival, C-reactive protein (CRP) levels, and the Japanese Orthopaedic Association (JOA) hip score were significantly different between the PMN-positive and PMN-negative group (p < 0.01). A BHA survival cut-off value of 3270 days was diagnostic for PMN positivity (sensitivity: 100%; specificity: 100%). The cut-off values for CRP and the JOA hip score were 0.43 mg/dl and 56 points, respectively. Four of 11 PMN-positive patients showed no clinical symptoms of infection (asymptomatic PMN-positive group). BHA survival, CRP levels, and JOA hip scores were significantly different between the asymptomatic PMN-positive and PMN-negative group (p < 0.05). A BHA survival cut-off of 3270 days was diagnostic for asymptomatic PMN positivity (sensitivity: 100%; specificity: 100%). The cut-off values for CRP and the JOA hip score were 0.43 mg/dl and 57 points, respectively.
Conclusion: Our findings suggest that some portion of rapid BHA prosthesis migration is caused by mild infection. Careful pathological examination should be performed to identify infection before removal of the BHA prosthesis in patients who develop migration within 9 years.
Figures


References
-
- Bateman JE. Single-assembly total hip prosthesis--preliminary report. 1974. Clin Orthop Relat Res. 1990;251:3–6. - PubMed
-
- D’Arcy J, Devas M. Treatment of fractures of the femoral neck by replacement with the Thompson prosthesis. J Bone Joint Surg Br. 1976;58(3):279–86. - PubMed
-
- Phillips TW. Thompson hemiarthroplasty and acetabular erosion. J Bone Joint Surg. 1989;71(6):913–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
