

Nationwide Hospitalization Trends in Adult Congenital Heart Disease Across 2003-2012
- PMID: 26786543
- PMCID: PMC4859356
- DOI: 10.1161/JAHA.115.002330
Nationwide Hospitalization Trends in Adult Congenital Heart Disease Across 2003-2012
Abstract
Background: We aimed to assess trends in hospitalization, outcomes, and resource utilization among patients admitted with adult congenital heart disease (ACHD).
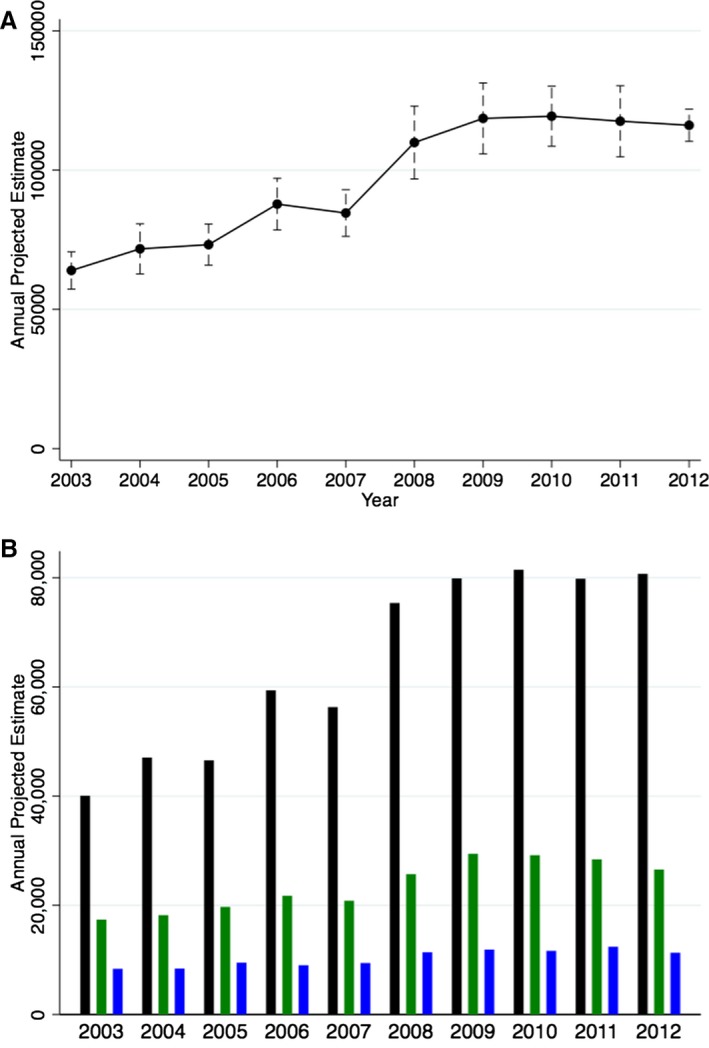
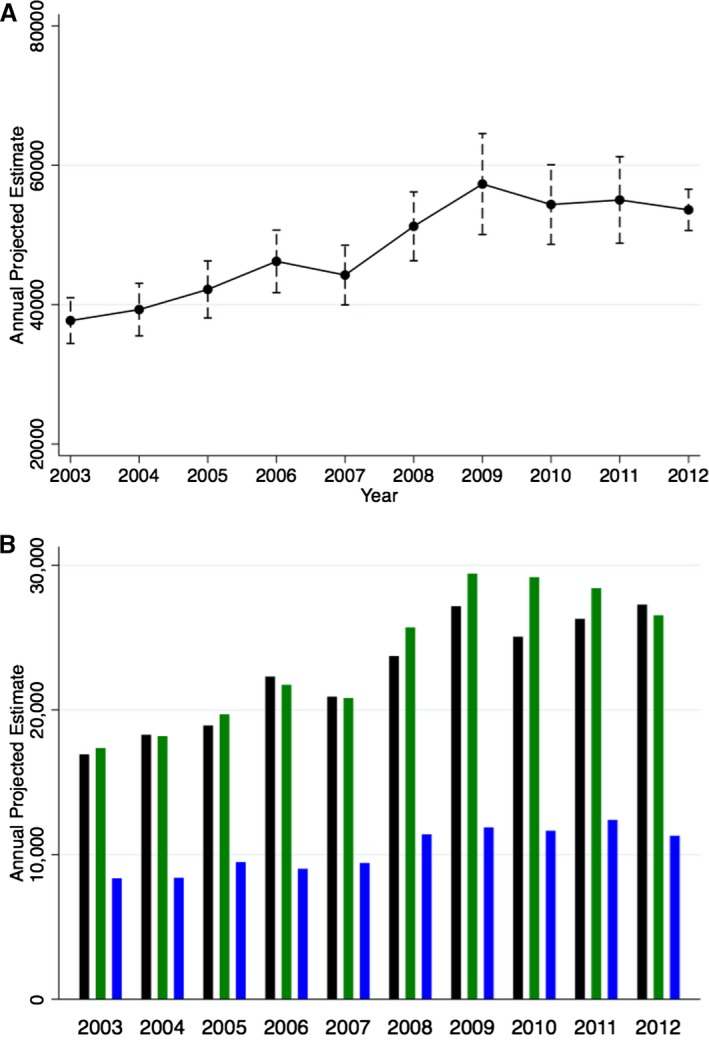
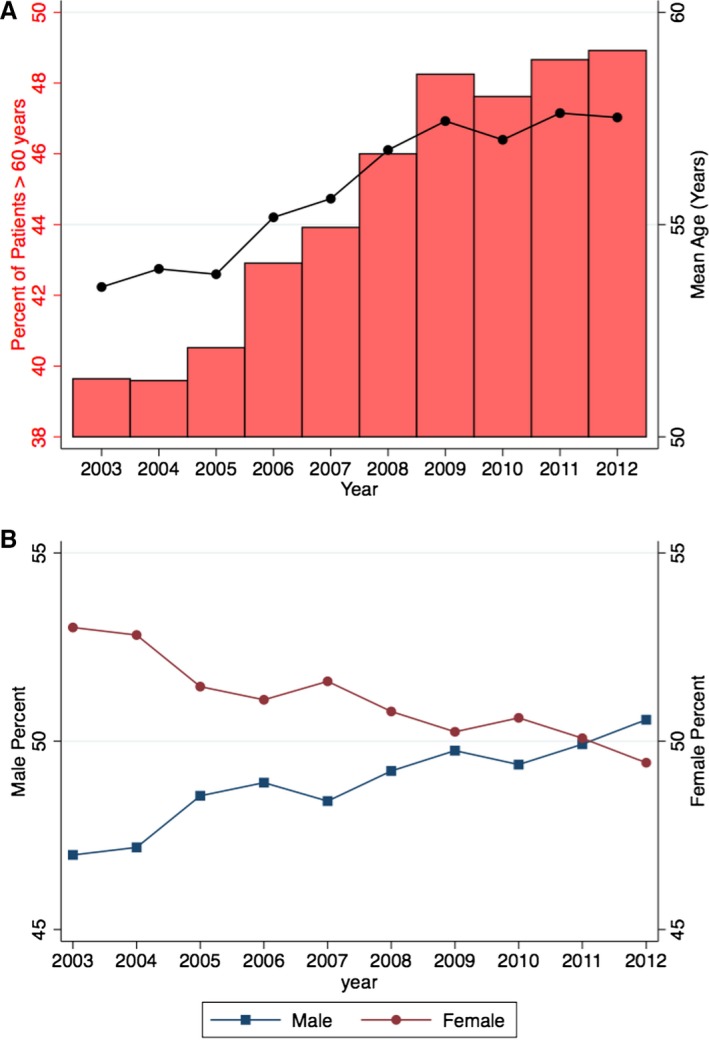
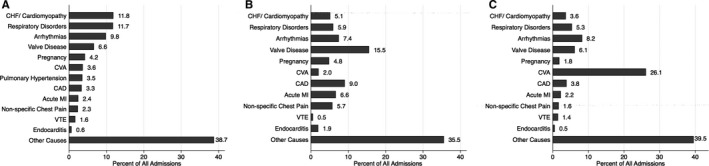
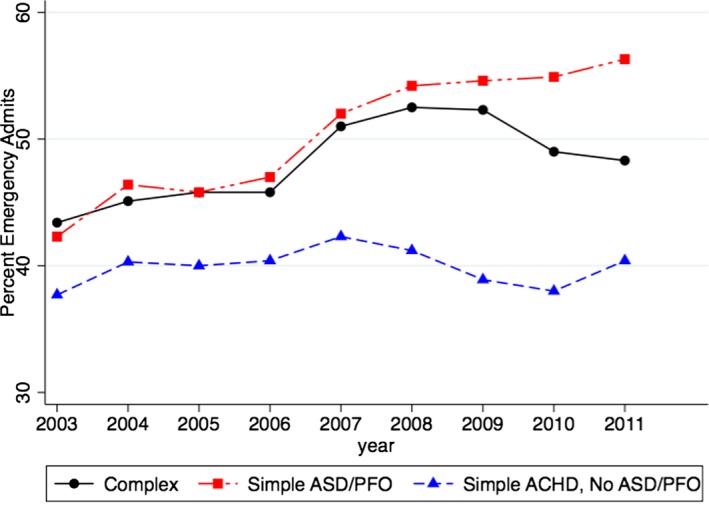
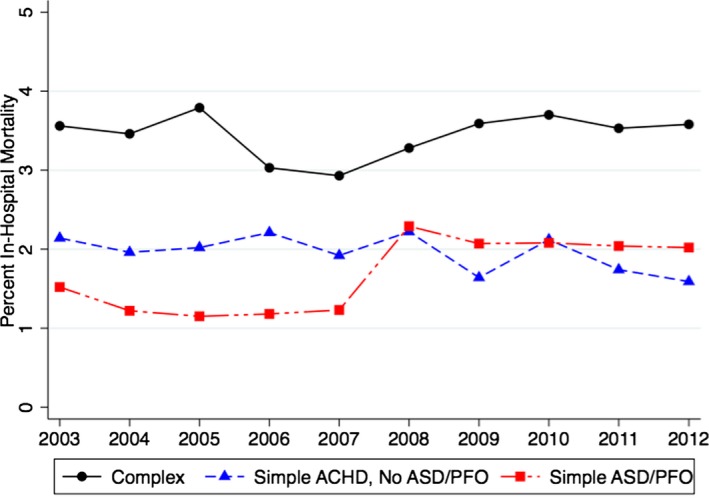
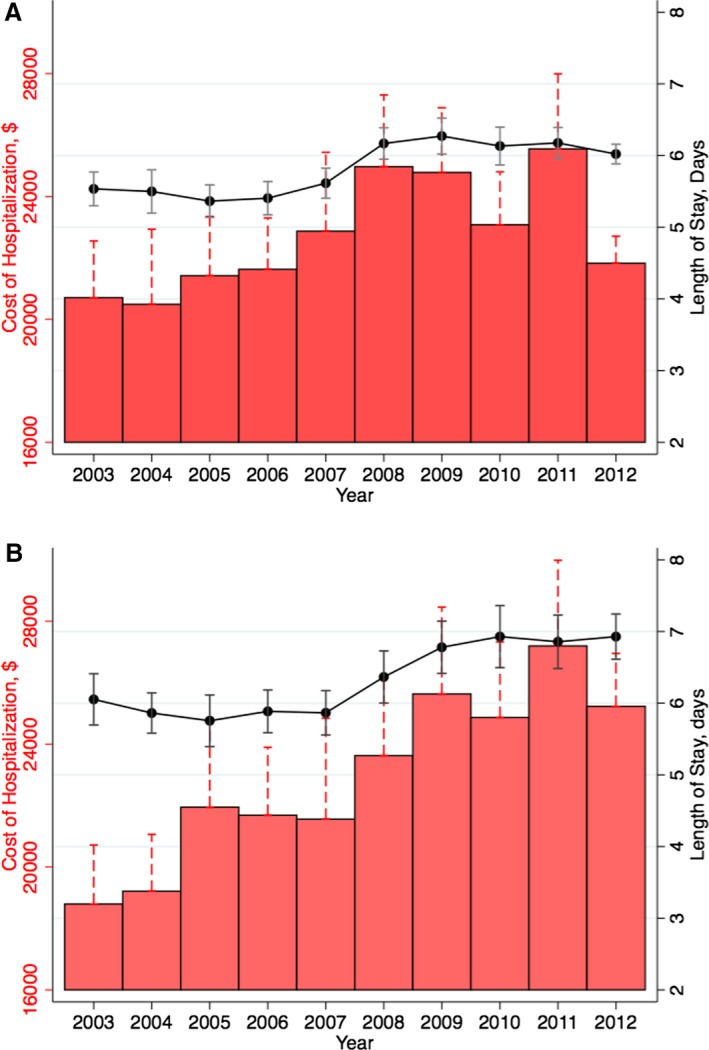
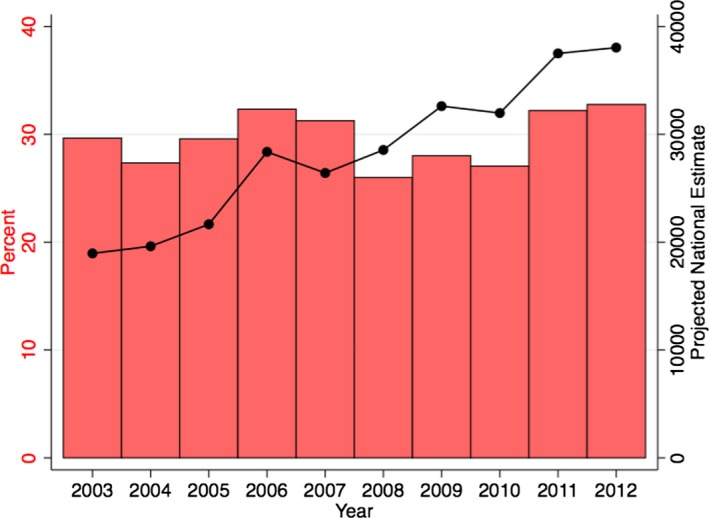
Methods and results: We used the 2003-2012 US Nationwide Inpatient Sample for this study. All admissions with an ACHD were identified using standard ICD codes. Resource utilization was assessed using length of stay, invasive procedure utilization, and cost of hospitalization. There was a significant increase in the number of both simple (101%) as well as complex congenital heart disease (53%)-related admissions across 2003-2012. In addition, there was a considerable increase in the prevalence of traditional cardiovascular risk factors including older age, along with a higher prevalence of hypertension, diabetes, smoking, obesity, chronic kidney disease, and peripheral arterial disease. Besides miscellaneous causes, congestive heart failure (11.8%), valve disease (15.5%), and cerebrovascular accident (26.1%) were the top causes of admission to the hospital among patients with complex ACHD, simple ACHD without atrial septal defects/patent foramen ovale and simple atrial septal defects/patent foramen ovale patients, respectively. In-hospital mortality has been relatively constant among patients with complex ACHD as well as simple ACHD without atrial septal defects/patent foramen ovale. However, there has been considerable increase in the average length of stay and cost of hospitalization among the ACHD patients during 2003-2012.
Conclusions: There has been a progressive increase in ACHD admissions across 2003-2012 in the United States, with increasing healthcare resource utilization among these patients. Moreover, there has been a change in the cardiovascular comorbidities of these patients, adding a layer of complexity in management of ACHD patients.
Keywords: adult congenital heart disease; cost of illness; hospital admission; length of stay; mortality; trends.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Warnes CA, Liberthson R, Danielson GK, Dore A, Harris L, Hoffman JI, Somerville J, Williams RG, Webb GD. Task force 1: the changing profile of congenital heart disease in adult life. J Am Coll Cardiol. 2001;37:1170–1175. - PubMed
-
- Baumgartner H. Geriatric congenital heart disease: a new challenge in the care of adults with congenital heart disease? Eur Heart J. 2014;35:683–685. - PubMed
-
- Opotowsky AR, Siddiqi OK, Webb GD. Trends in hospitalizations for adults with congenital heart disease in the U.S. J Am Coll Cardiol. 2009;54:460–467. - PubMed
-
- Healthcare utilization project. Agency for Healthcare Research & Quality. Available at: http://www.hcup-us.ahrq.gov/db/nation/nis/nisdde.jsp. Accessed May 5, 2015.
-
- Healthcare Cost and Utilization Project (HCUP) . HCUP Comorbidity Software 1‐14‐2013. Rockville, MD: Agency for Healthcare Research and Quality; 2013. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
