

Gene promoter methylation signature predicts survival of head and neck squamous cell carcinoma patients
- PMID: 26786582
- PMCID: PMC4846111
- DOI: 10.1080/15592294.2015.1137414
Gene promoter methylation signature predicts survival of head and neck squamous cell carcinoma patients
Abstract
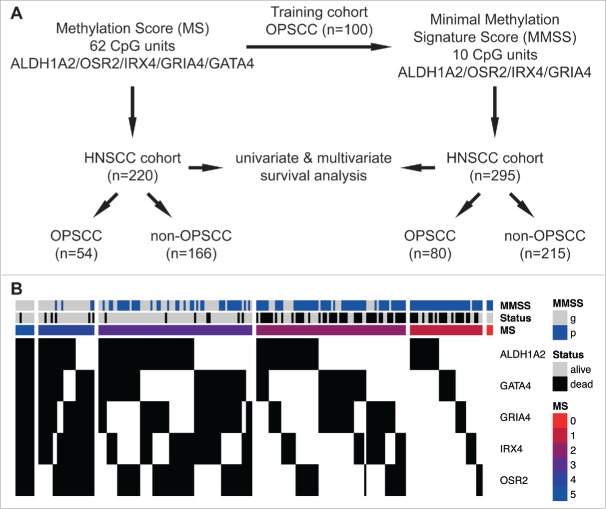
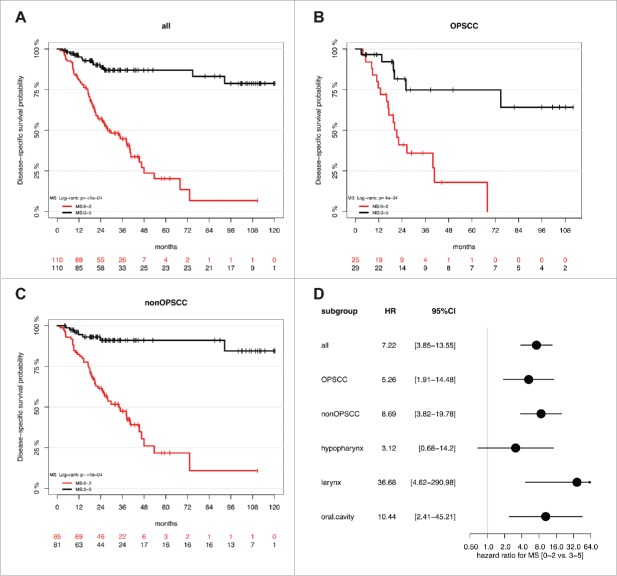
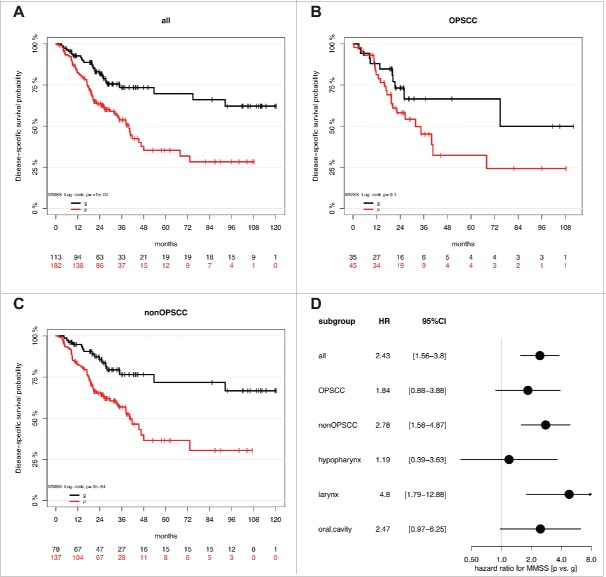
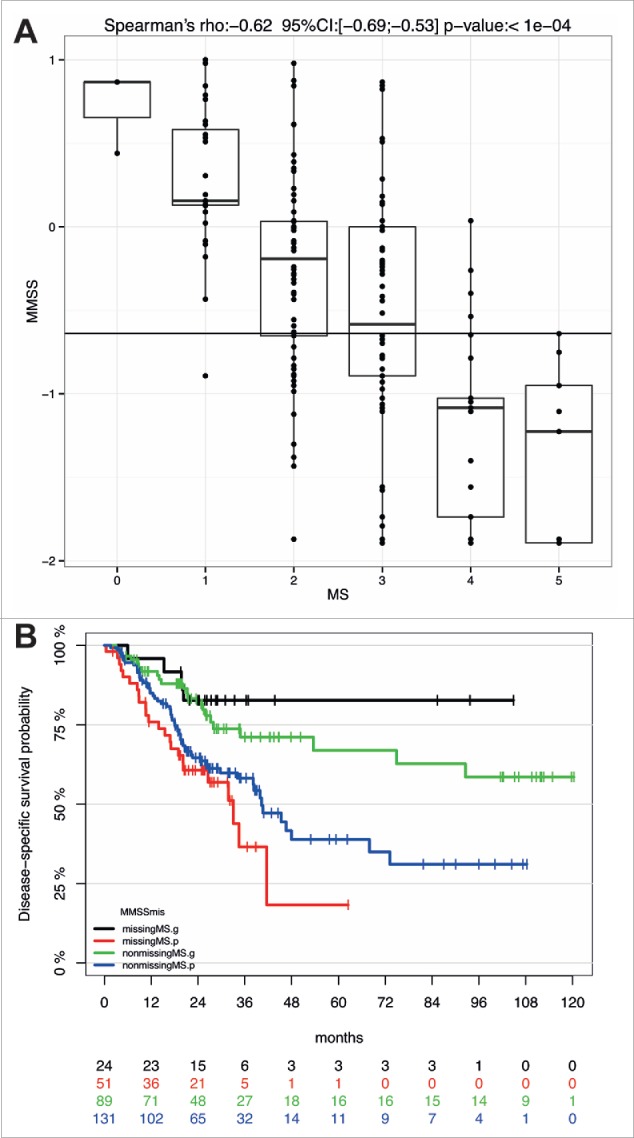
Infection with high-risk types of human papilloma virus (HPV) is currently the best-established prognostic marker for head and neck squamous cell carcinoma (HNSCC), one of the most common and lethal human malignancies worldwide. Clinical trials have been launched to address the concept of treatment de-escalation for HPV-positive HNSCC with the final aim to reduce treatment related toxicity and debilitating long-term impacts on the quality of life. However, HPV-related tumors are mainly restricted to oropharyngeal SCC (OPSCC) and there is an urgent need to establish reliable biomarkers for all patients at high risk for treatment failure. A patient cohort (n = 295) with mainly non-OPSCC (72.9%) and a low prevalence of HPV16-related tumors (8.8%) was analyzed by MassARRAY to determine a previously established prognostic methylation score (MS). Kaplan-Meier revealed a highly significant correlation between a high MS and a favorable survival for OPSCC (P = 0.0004) and for non-OPSCC (P<0.0001), which was confirmed for all HNSCC by multivariate Cox regression models (HR: 9.67, 95% CI [4.61-20.30], P<0.0001). Next, we established a minimal methylation signature score (MMSS), which consists of ten most informative of the originally 62 CpG units used for the MS. The prognostic value of the MMSS was confirmed by Kaplan-Meier analysis for all HNSCC (P<0.0001) and non-OPSCC (P = 0.0002), and was supported by multivariate Cox regression models for all HNSCC (HR: 2.15, 95% CI [1.36-3.41], P = 0.001). In summary, the MS and the MMSS exhibit an excellent performance as prognosticators for survival, which is not limited by the anatomical site, and both could be implemented in future clinical trials.
Keywords: DNA methylation; HNSCC; HPV; MassARRAY; OPSCC; head and neck cancer; squamous cell carcinoma.
Figures
References
-
- Leemans CR, Braakhuis BJ, Brakenhoff RH. The molecular biology of head and neck cancer. Nat Rev Cancer 2011; 11:9-22; PMID:21160525; http://dx.doi.org/ 10.1038/nrc2982 - DOI - PubMed
-
- Ndiaye C, Mena M, Alemany L, Arbyn M, Castellsague X, Laporte L, Bosch FX, de Sanjose S, Trottier H. HPV DNA, E6/E7 mRNA, and p16INK4a detection in head and neck cancers: a systematic review and meta-analysis. Lancet Oncol 2014; 15:1319-31; PMID:25439690; http://dx.doi.org/ 10.1016/S1470-2045(14)70471-1 - DOI - PubMed
-
- Mehanna H, Beech T, Nicholson T, El-Hariry I, McConkey C, Paleri V, Roberts S. Prevalence of human papillomavirus in oropharyngeal and nonoropharyngeal head and neck cancer–systematic review and meta-analysis of trends by time and region. Head Neck 2013; 35:747-55; PMID:22267298; http://dx.doi.org/ 10.1002/hed.22015 - DOI - PubMed
-
- Network CGA. Comprehensive genomic characterization of head and neck squamous cell carcinomas. Nature 2015; 517:576-82; PMID:25631445; http://dx.doi.org/ 10.1038/nature14129 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials