

T cells from patients with Candida sepsis display a suppressive immunophenotype
- PMID: 26786705
- PMCID: PMC4719210
- DOI: 10.1186/s13054-016-1182-z
T cells from patients with Candida sepsis display a suppressive immunophenotype
Abstract
Background: Despite appropriate therapy, Candida bloodstream infections are associated with a mortality rate of approximately 40%. In animal models, impaired immunity due to T cell exhaustion has been implicated in fungal sepsis mortality. The purpose of this study was to determine potential mechanisms of fungal-induced immunosuppression via immunophenotyping of circulating T lymphocytes from patients with microbiologically documented Candida bloodstream infections.
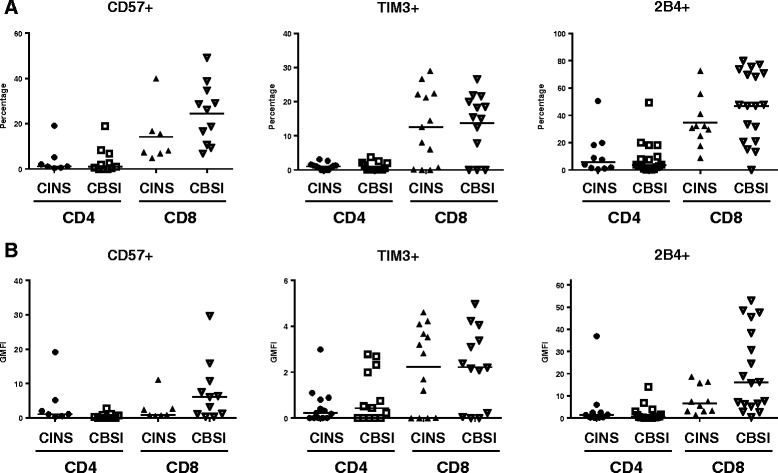
Methods: Patients with blood cultures positive for any Candida species were studied. Non-septic critically ill patients with no evidence of bacterial or fungal infection were controls. T cells were analyzed via flow cytometry for cellular activation and for expression of positive and negative co-stimulatory molecules. Both the percentages of cells expressing particular immunophenotypic markers as well as the geometric mean fluorescence intensity (GMFI), a measure of expression of the number of receptors or ligands per cell, were quantitated.
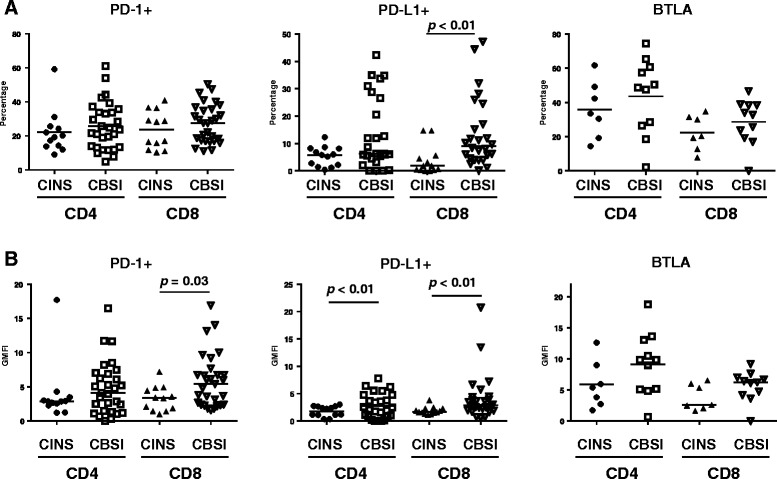
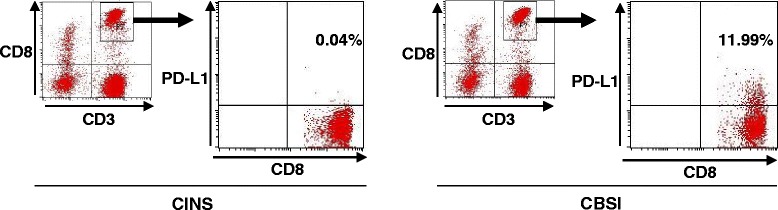
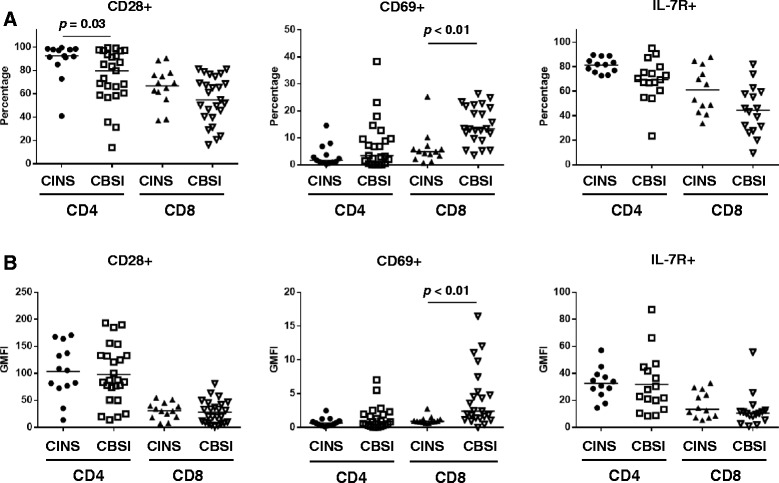
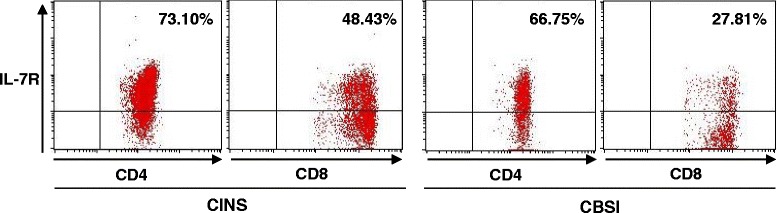
Results: Twenty-seven patients with Candida bloodstream infections and 16 control patients were studied. Compared to control patients, CD8 T cells from patients with Candidemia had evidence of cellular activation as indicated by increased CD69 expression while CD4 T cells had decreased expression of the major positive co-stimulatory molecule CD28. CD4 and CD8 T cells from patients with Candidemia expressed markers typical of T cell exhaustion as indicated by either increased percentages of or increased MFI for programmed cell death 1 (PD-1) or its ligand (PD-L1).
Conclusions: Circulating immune effector cells from patients with Candidemia display an immunophenotype consistent with immunosuppression as evidenced by T cell exhaustion and concomitant downregulation of positive co-stimulatory molecules. These findings may help explain why patients with fungal sepsis have a high mortality despite appropriate antifungal therapy. Development of immunoadjuvants that reverse T cell exhaustion and boost host immunity may offer one way to improve outcome in this highly lethal disorder.
Figures
Comment in
-
From bedside to bench: the missing brick for patients with fungal sepsis.Crit Care. 2016 Jun 21;20(1):191. doi: 10.1186/s13054-016-1378-2. Crit Care. 2016. PMID: 27323797 Free PMC article. No abstract available.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
