

Feasibility of eliminating visceral leishmaniasis from the Indian subcontinent: explorations with a set of deterministic age-structured transmission models
- PMID: 26787302
- PMCID: PMC4717541
- DOI: 10.1186/s13071-016-1292-0
Feasibility of eliminating visceral leishmaniasis from the Indian subcontinent: explorations with a set of deterministic age-structured transmission models
Abstract
Background: Visceral leishmaniasis (VL) is a neglected tropical disease transmitted by sandflies. On the Indian subcontinent (ISC), VL is targeted for elimination as a public health problem by 2017. In the context of VL, the elimination target is defined as an annual VL incidence of <1 per 10,000 capita at (sub-)district level. Interventions focus on vector control, surveillance and on diagnosing and treating VL cases. Many endemic areas have not yet achieved optimal control due to logistical, biological as well as technical challenges. We used mathematical modelling to quantify VL transmission dynamics and predict the feasibility of achieving the VL elimination target with current control strategies under varying assumptions about the reservoir of infection in humans.
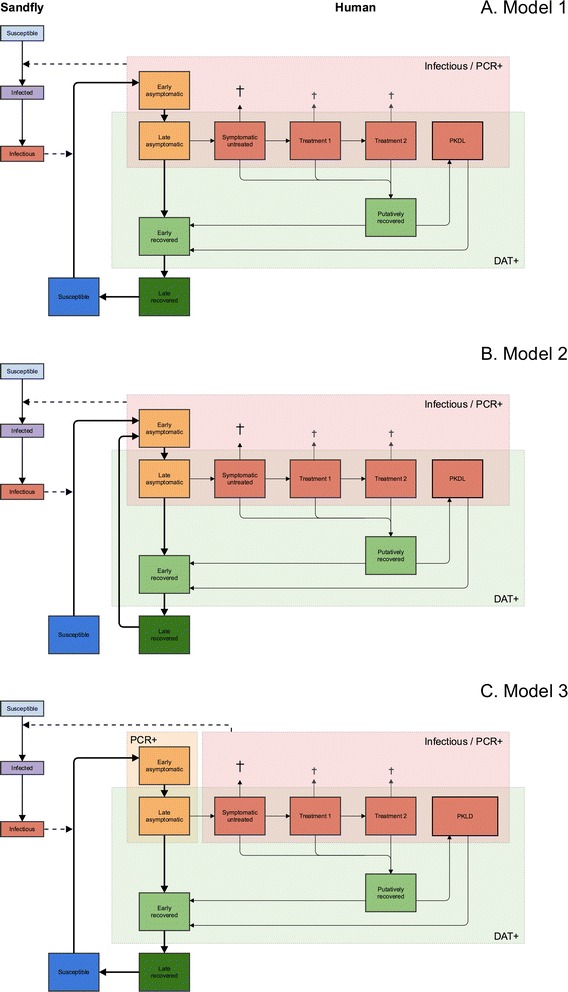
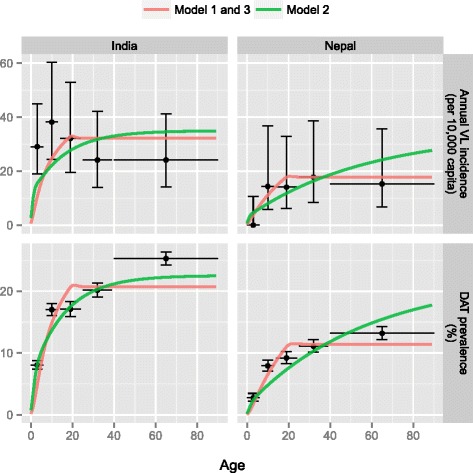
Methods: We developed three deterministic age-structured transmission models with different main reservoirs of infection in humans: asymptomatic infections (model 1), reactivation of infection after initial infection (model 2), and post kala-azar dermal leishmaniasis (PKDL; model 3). For each model, we defined four sub-variants based on different assumptions about the duration of immunity and age-patterns in exposure to sandflies. All 12 model sub-variants were fitted to data from the KalaNet study in Bihar (India) and Nepal, and the best sub-variant was selected per model. Predictions were made for optimal and sub-optimal indoor residual spraying (IRS) effectiveness for three different levels of VL endemicity.
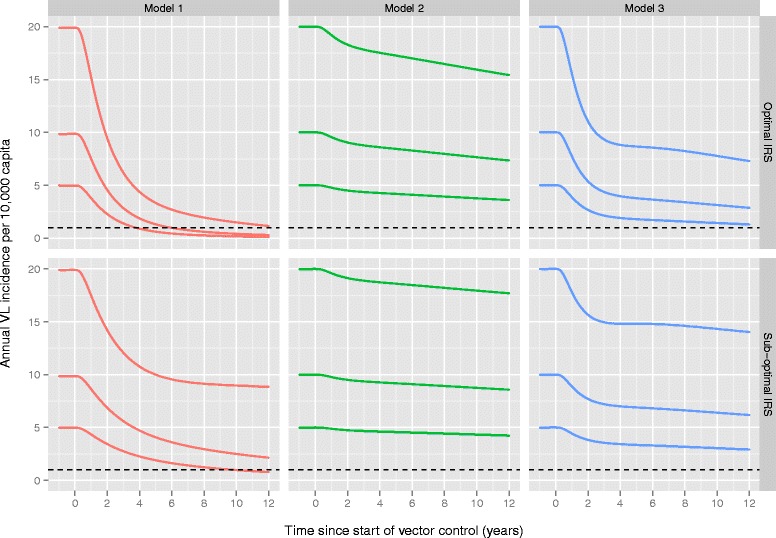
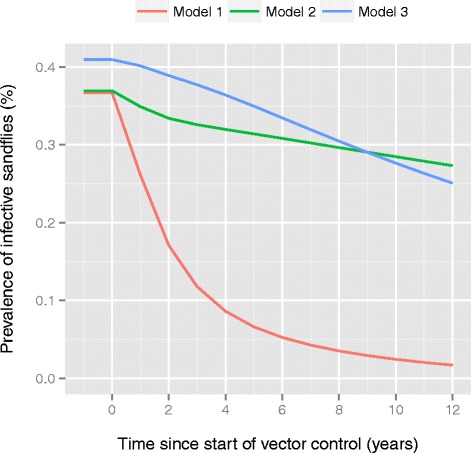
Results: Structurally different models explained the KalaNet data equally well. However, the predicted impact of IRS varied substantially between models, such that a conclusion about reaching the VL elimination targets for the ISC heavily depends on assumptions about the main reservoir of infection in humans: asymptomatic cases, recovered (immune) individuals that reactivate, or PKDL cases.
Conclusions: Available data on the impact of IRS so far suggest one model is probably closest to reality (model 1). According to this model, elimination of VL (incidence of <1 per 10,000) by 2017 is only feasible in low and medium endemic settings with optimal IRS. In highly endemic settings and settings with sub-optimal IRS, additional interventions will be required.
Figures
References
-
- Savioli L, Daumerie D, World Health Organization . First WHO report on neglected tropical diseases: working to overcome the global impact of neglected tropical diseases. Geneva Switzerland: World Health; 2010. pp. 1–184.
-
- World Health Organization . Leishmaniasis Fact sheet N°375. Geneva, Switzerland: WHO Media Centre; 2015.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
