

Aortic valve surgery and survival in patients with moderate or severe aortic stenosis and left ventricular dysfunction
- PMID: 26787441
- PMCID: PMC5841220
- DOI: 10.1093/eurheartj/ehv701
Aortic valve surgery and survival in patients with moderate or severe aortic stenosis and left ventricular dysfunction
Abstract
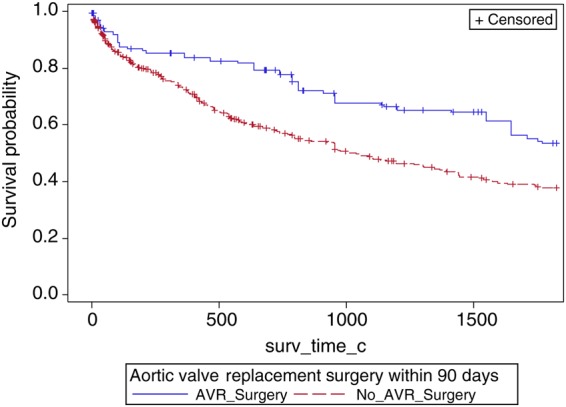
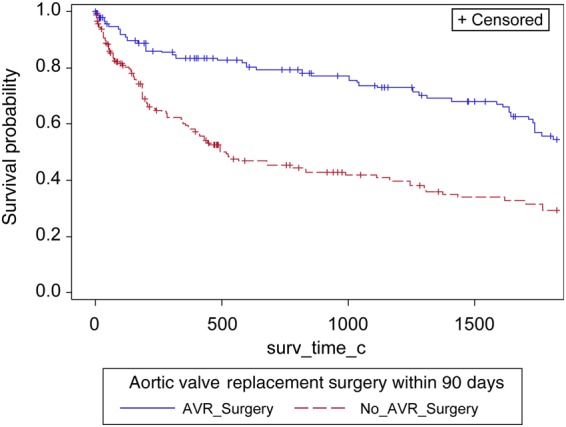
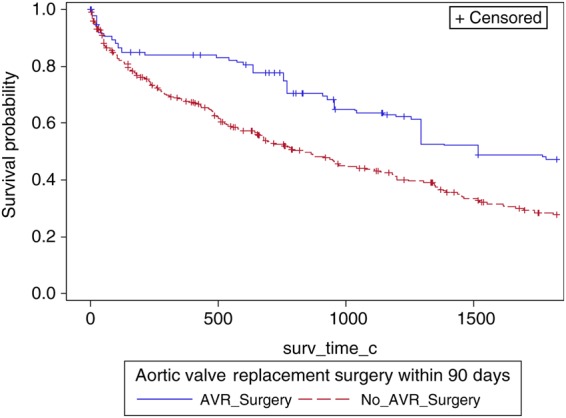
Aims: We aimed to determine the frequency of aortic valve surgery (AVR) with or without coronary artery bypass grafting (CABG), among patients with moderate/severe aortic stenosis (AS) and left ventricular systolic dysfunction (LVSD), and its relationship with survival.
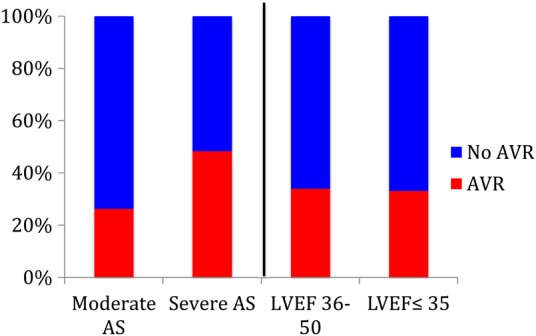
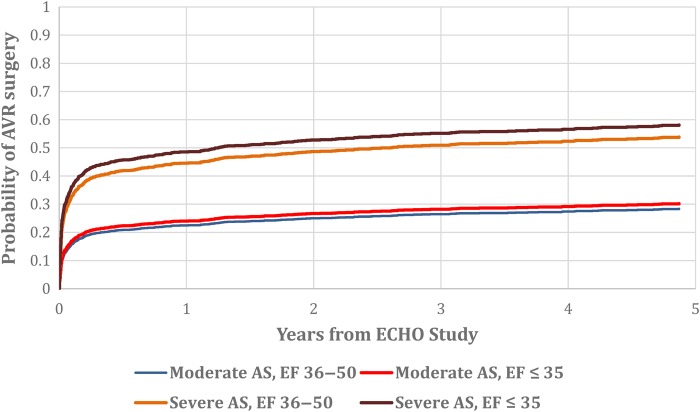
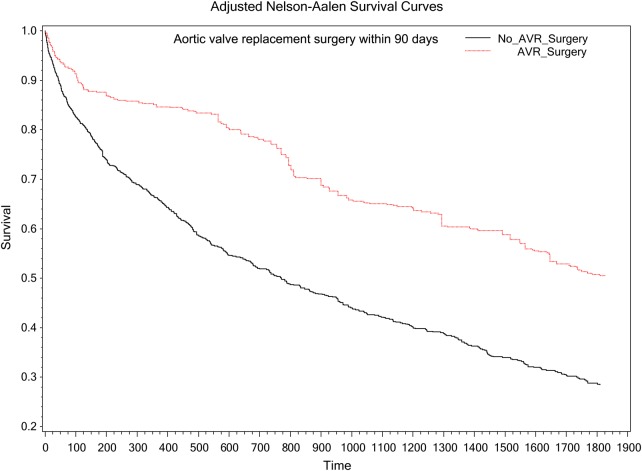
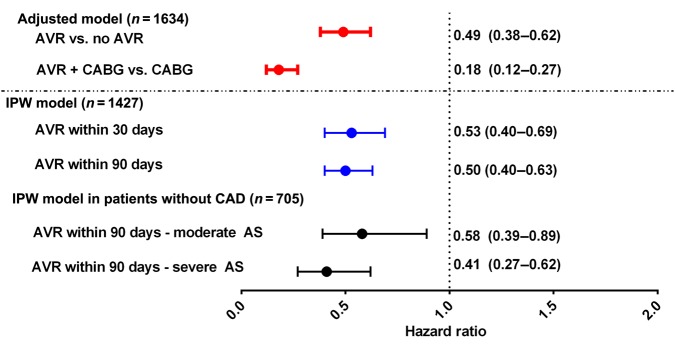
Methods and results: The Duke Echocardiographic Database (N = 132 804) was queried for patients with mean gradient ≥25 mmHg and/or peak velocity ≥3 m/s and LVSD (left ventricular ejection fraction ≤50%) from 1 January 1995-28 February 2014. For analyses purposes, AS was defined both by mean gradient and calculated aortic valve area (AVA) criteria. Time-dependent indicators of AVR in multivariable Cox models were used to assess the relationship of AVR and all-cause mortality. A total of 1634 patients had moderate (N = 1090, 67%) or severe (N = 544, 33%) AS by mean gradient criteria. Overall, 287 (26%) patients with moderate AS and 263 (48%) patients with severe AS underwent AVR within 5 years of the qualifying echo. There were 863 (53%) deaths observed up to 5 years following index echo. After multivariable adjustment in an inverse probability weighted regression model, AVR was associated with higher 5-year survival amongst patients with moderate AS and severe AS whether classified by AVA or mean gradient criteria. Over all, AVR ± CABG compared with medical therapy was associated with significantly lower mortality [hazard ratio, HR = 0.49 (0.38, 0.62), P < 0.0001]. Compared with CABG alone, CABG + AVR was associated with better survival [HR = 0.18 (0.12, 0.27), P < 0.0001].
Conclusions: In patients with moderate/severe AS and LVSD, mortality is substantial and amongst those selected for surgery, AVR with or without CABG is associated with higher survival. Research is required to understand factors contributing to current practice patterns and the possible utility of transcatheter approaches in this high-risk cohort.
Keywords: Moderate aortic stenosis; aortic valve surgery; left ventricular systolic dysfunction; severe aortic stenosis; survival.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2016. For permissions please email: journals.permissions@oup.com.
Figures
Similar articles
-
The prognostic impact of concomitant coronary artery bypass grafting during aortic valve surgery: implications for revascularization in the transcatheter era.J Thorac Cardiovasc Surg. 2015 Feb;149(2):451-60. doi: 10.1016/j.jtcvs.2014.08.073. Epub 2014 Sep 17. J Thorac Cardiovasc Surg. 2015. PMID: 25308117
-
Moderate aortic stenosis in coronary artery bypass grafting patients more than 70 years of age: to replace or not to replace?Ann Thorac Surg. 2010 Nov;90(5):1495-9; discussion 1499-500. doi: 10.1016/j.athoracsur.2010.06.036. Ann Thorac Surg. 2010. PMID: 20971247
-
Aortic valve replacement: a safe and durable option in patients with impaired left ventricular systolic function.Eur J Cardiothorac Surg. 2006 Feb;29(2):133-8. doi: 10.1016/j.ejcts.2005.11.028. Eur J Cardiothorac Surg. 2006. PMID: 16386914
-
Aortic valve replacement after previous coronary artery bypass grafting.Ann Thorac Surg. 1996 Nov;62(5):1424-30. doi: 10.1016/0003-4975(96)00635-2. Ann Thorac Surg. 1996. PMID: 8893579 Review.
-
Management of mild to moderate aortic stenosis at the time of coronary artery bypass grafting.J Heart Valve Dis. 2002 Jan;11 Suppl 1:S45-9. J Heart Valve Dis. 2002. PMID: 11843520 Review.
Cited by
-
Moderate Aortic Valve Stenosis with Left Ventricular Systolic Dysfunction: Potential Role of Early Aortic Valve Replacement.Korean Circ J. 2020 Sep;50(9):801-803. doi: 10.4070/kcj.2020.0301. Korean Circ J. 2020. PMID: 32812409 Free PMC article. No abstract available.
-
Left ventricular hypertrophy, diastolic dysfunction and right ventricular load predict outcome in moderate aortic stenosis.Front Cardiovasc Med. 2023 Jan 10;9:1101493. doi: 10.3389/fcvm.2022.1101493. eCollection 2022. Front Cardiovasc Med. 2023. PMID: 36704453 Free PMC article.
-
Evolving Indications of Transcatheter Aortic Valve Replacement-Where Are We Now, and Where Are We Going.J Clin Med. 2022 May 30;11(11):3090. doi: 10.3390/jcm11113090. J Clin Med. 2022. PMID: 35683476 Free PMC article. Review.
-
Left Ventricular Systolic Dysfunction in Aortic Stenosis: Pathophysiology, Diagnosis, Management, and Future Directions.Struct Heart. 2022 Sep 15;6(5):100089. doi: 10.1016/j.shj.2022.100089. eCollection 2022 Oct. Struct Heart. 2022. PMID: 37288060 Free PMC article. Review.
-
Outcomes with moderate aortic stenosis and impaired left ventricular function: prelude to a randomized trial?J Thorac Dis. 2017 Oct;9(10):3529-3532. doi: 10.21037/jtd.2017.09.16. J Thorac Dis. 2017. PMID: 29268333 Free PMC article. No abstract available.
References
-
- Rankin JS, Hammill BG, Ferguson TB Jr, Glower DD, O'Brien SM, DeLong ER, Peterson ED, Edwards FH. Determinants of operative mortality in valvular heart surgery. J Thoracic Cardiovasc Surg 2006;131:547–557. - PubMed
-
- Iung B, Baron G, Butchart EG, Delahaye F, Gohlke-Barwolf C, Levang OW, Tornos P, Vanoverschelde JL, Vermeer F, Boersma E, Ravaud P, Vahanian A. A prospective survey of patients with valvular heart disease in Europe: The euro heart survey on valvular heart disease. Eur Heart J 2003;24:1231–1243. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton RA, O'Gara PT, Ruiz CE, Skubas NJ, Sorajja P, Sundt TM III, Thomas JD, Members AATF. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American college of cardiology/American heart association task force on practice guidelines. Circulation. 2014;129:e521–e643. - PubMed
-
- Ross J., Jr Afterload mismatch in aortic and mitral valve disease: implications for surgical therapy. J Am College Cardiol 1985;5:811–826. - PubMed
-
- Wisenbaugh T, Booth D, DeMaria A, Nissen S, Waters J. Relationship of contractile state to ejection performance in patients with chronic aortic valve disease. Circulation. 1986;73:47–53. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
