

Clinical Utility and Safety of a Model-Based Patient-Tailored Dose of Vancomycin in Neonates
- PMID: 26787690
- PMCID: PMC4808207
- DOI: 10.1128/AAC.02214-15
Clinical Utility and Safety of a Model-Based Patient-Tailored Dose of Vancomycin in Neonates
Abstract
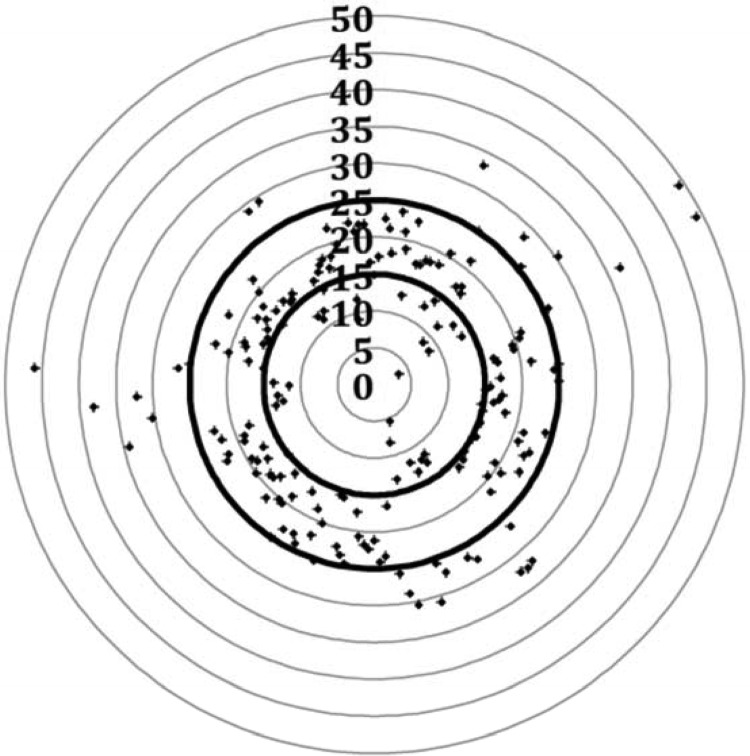
Pharmacokinetic modeling has often been applied to evaluate vancomycin pharmacokinetics in neonates. However, clinical application of the model-based personalized vancomycin therapy is still limited. The objective of the present study was to evaluate the clinical utility and safety of a model-based patient-tailored dose of vancomycin in neonates. A model-based vancomycin dosing calculator, developed from a population pharmacokinetic study, has been integrated into the routine clinical care in 3 neonatal intensive care units (Robert Debré, Cochin Port Royal, and Clocheville hospitals) between 2012 and 2014. The target attainment rate, defined as the percentage of patients with a first therapeutic drug monitoring serum vancomycin concentration achieving the target window of 15 to 25 mg/liter, was selected as an endpoint for evaluating the clinical utility. The safety evaluation was focused on nephrotoxicity. The clinical application of the model-based patient-tailored dose of vancomycin has been demonstrated in 190 neonates. The mean (standard deviation) gestational and postnatal ages of the study population were 31.1 (4.9) weeks and 16.7 (21.7) days, respectively. The target attainment rate increased from 41% to 72% without any case of vancomycin-related nephrotoxicity. This proof-of-concept study provides evidence for integrating model-based antimicrobial therapy in neonatal routine care.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
