Polymicrobial Purulent Pericarditis Probably caused by a Broncho-Lymph Node-Pericardial Fistula in a Patient with Tuberculous Lymphadenitis
- PMID: 26788411
- PMCID: PMC4716279
- DOI: 10.3947/ic.2015.47.4.261
Polymicrobial Purulent Pericarditis Probably caused by a Broncho-Lymph Node-Pericardial Fistula in a Patient with Tuberculous Lymphadenitis
Abstract
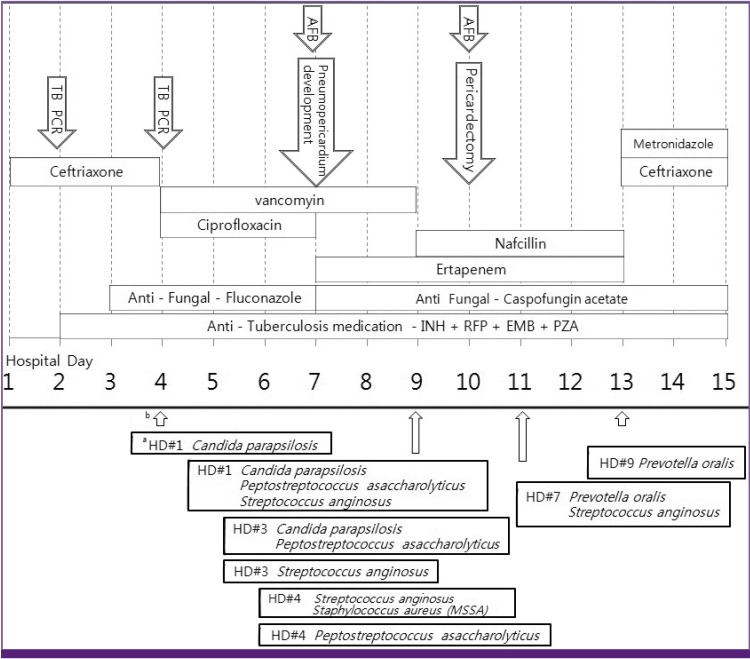
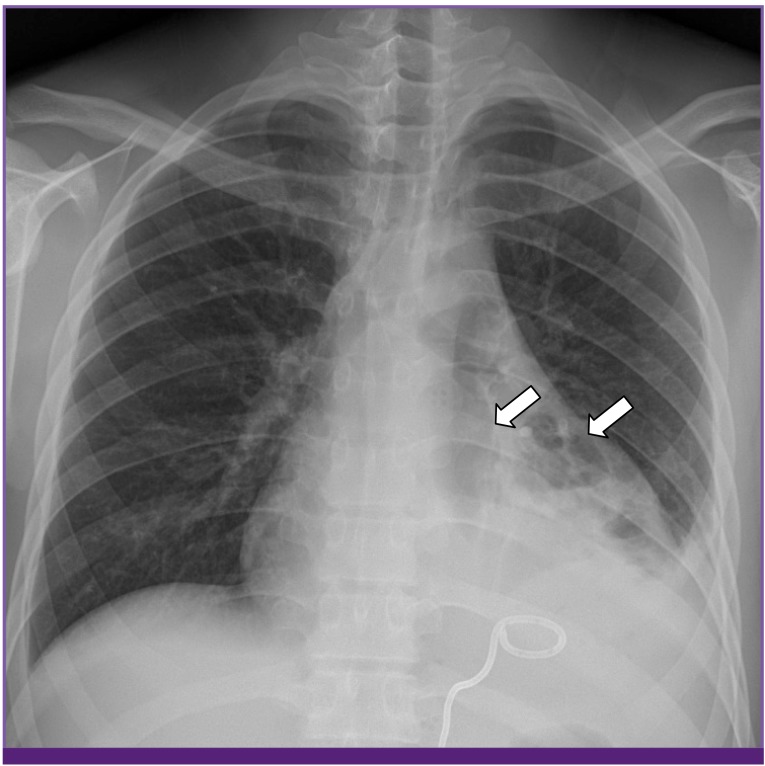
Purulent pericarditis is a rare condition with a high mortality rate. We report a case of purulent pericarditis subsequently caused by Candida parapsilosis, Peptostreptococcus asaccharolyticus, Streptococcus anginosus, Staphylococcus aureus, Prevotella oralis, and Mycobacterium tuberculosis in a previously healthy 17-year-old boy with mediastinal tuberculous lymphadenitis. The probable route of infection was a bronchomediastinal lymph node-pericardial fistula. The patient improved with antibiotic, antifungal, and antituberculous medication in addition to pericardiectomy.
Keywords: Bronchial fistula; Pericarditis; Polymicrobial infection; Tuberculous lymphadenitis; Tuberculous pericarditis.
Figures



Similar articles
-
Partial pericardiectomy for refractory acute tuberculous pericarditis: A case report.Int J Surg Case Rep. 2023 May;106:108239. doi: 10.1016/j.ijscr.2023.108239. Epub 2023 Apr 19. Int J Surg Case Rep. 2023. PMID: 37087940 Free PMC article.
-
Purulent Streptococcus intermedius Pericarditis in the Setting of Histoplasma Mediastinal Lymphadenitis: A Case Report and Literature Review.Cureus. 2024 Jun 18;16(6):e62626. doi: 10.7759/cureus.62626. eCollection 2024 Jun. Cureus. 2024. PMID: 39027746 Free PMC article.
-
Purulent pericarditis secondary to Candida parapsilosis and Peptostreptococcus species.Can J Cardiol. 1998 Jan;14(1):85-6. Can J Cardiol. 1998. PMID: 9487278
-
Bacterial pericarditis: diagnosis and management.Am J Cardiovasc Drugs. 2005;5(2):103-12. doi: 10.2165/00129784-200505020-00004. Am J Cardiovasc Drugs. 2005. PMID: 15725041 Review.
-
Purulent pericarditis caused by Candida species: case report and review.Clin Infect Dis. 1995 Jul;21(1):182-7. doi: 10.1093/clinids/21.1.182. Clin Infect Dis. 1995. PMID: 7578728 Review.
Cited by
-
Septic Shock, Renal Abscess, and Bacteremia Due to Peptoniphilus asaccharolyticus in a Woman with Nephrosis and Diabetes Mellitus: Case Report and Literature Review.Infect Drug Resist. 2022 Mar 4;15:831-836. doi: 10.2147/IDR.S353966. eCollection 2022. Infect Drug Resist. 2022. PMID: 35281574 Free PMC article.
-
Fungal Pericarditis-A Systematic Review of 101 Cases.Microorganisms. 2025 Mar 21;13(4):707. doi: 10.3390/microorganisms13040707. Microorganisms. 2025. PMID: 40284544 Free PMC article. Review.
-
Candida pericarditis presenting with cardiac tamponade and multiple organ failure after combined damage control thoracotomy and laparotomy with splenectomy in a trauma patient: Case report and review of literature.Trauma Case Rep. 2021 Dec 8;37:100564. doi: 10.1016/j.tcr.2021.100564. eCollection 2022 Feb. Trauma Case Rep. 2021. PMID: 34917734 Free PMC article.
-
Video-assisted thoracoscopic surgery for the treatment of mediastinal lymph node tuberculous abscesses.J Huazhong Univ Sci Technolog Med Sci. 2017 Dec;37(6):849-854. doi: 10.1007/s11596-017-1816-7. Epub 2017 Dec 21. J Huazhong Univ Sci Technolog Med Sci. 2017. PMID: 29270742
References
-
- Maisch B, Seferović PM, Ristić AD, Erbel R, Rienmüller R, Adler Y, Tomkowski WZ, Thiene G, Yacoub MH Task Force on the Diagnosis and Management of Pricardial Diseases of the European Society of Cardiology. Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European society of cardiology. Eur Heart J. 2004;25:587–610. - PubMed
-
- Shiber JR. Purulent pericarditis: Acute infections and chronic complications. Hosp Physician. 2008;44:9–18.
-
- Ferreira dos Santos L, Moreira D, Ribeiro P, Rodrigues B, Correia E, Nunes L, Sequeira M, Albuquerque A, Barros I, Saraiva JP, Santos O. Purulent pericarditis: a rare diagnosis. Rev Port Cardiol. 2013;32:721–727. - PubMed
-
- Rubin RH, Moellering RC., Jr Clinical, microbiologic and therapeutic aspects of purulent pericarditis. Am J Med. 1975;59:68–78. - PubMed
-
- Parsons R, Argoud G, Palmer DL. Mixed bacterial infection of the pericardium. South Med J. 1983;76:1046–1048. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources