

Artemisinin-Based Combination Therapy Versus Quinine or Other Combinations for Treatment of Uncomplicated Plasmodium falciparum Malaria in the Second and Third Trimester of Pregnancy: A Systematic Review and Meta-Analysis
- PMID: 26788543
- PMCID: PMC4716351
- DOI: 10.1093/ofid/ofv170
Artemisinin-Based Combination Therapy Versus Quinine or Other Combinations for Treatment of Uncomplicated Plasmodium falciparum Malaria in the Second and Third Trimester of Pregnancy: A Systematic Review and Meta-Analysis
Abstract
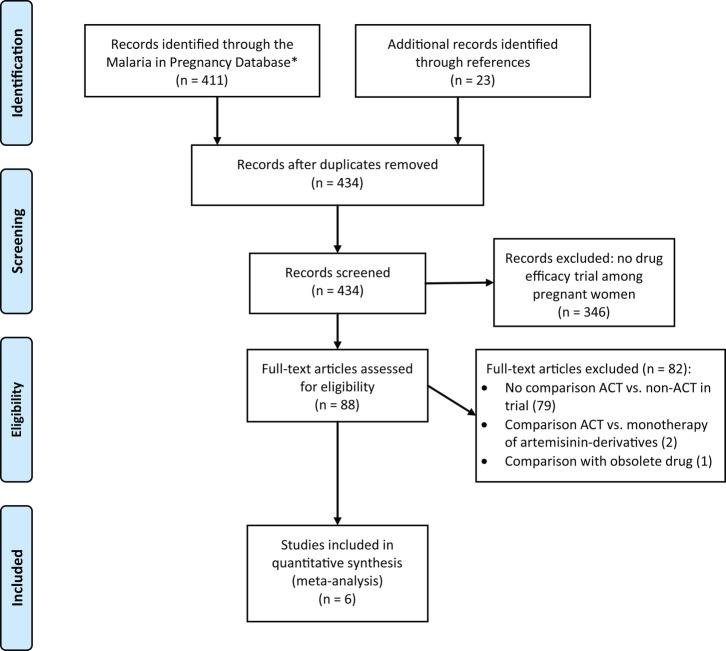
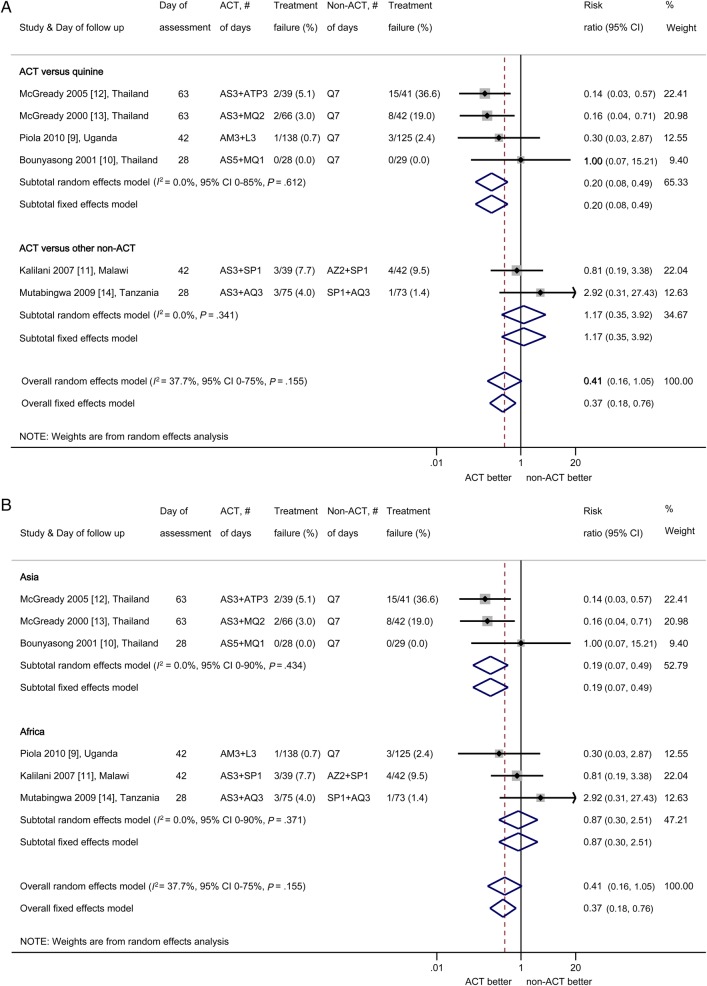
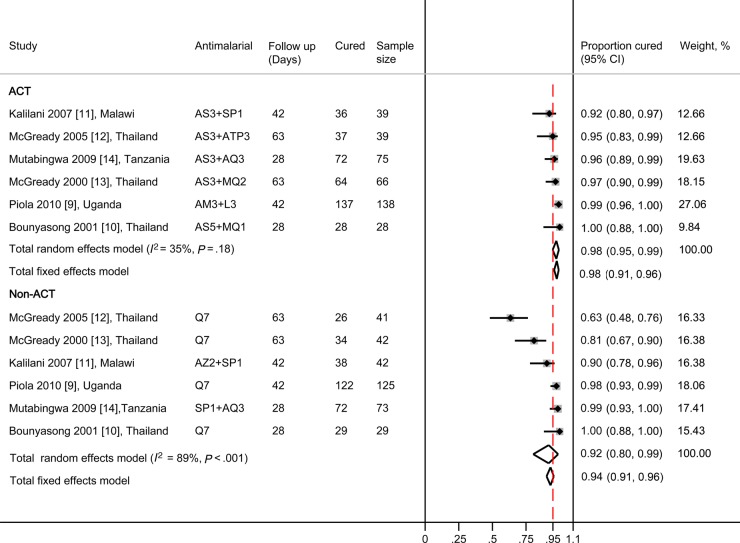
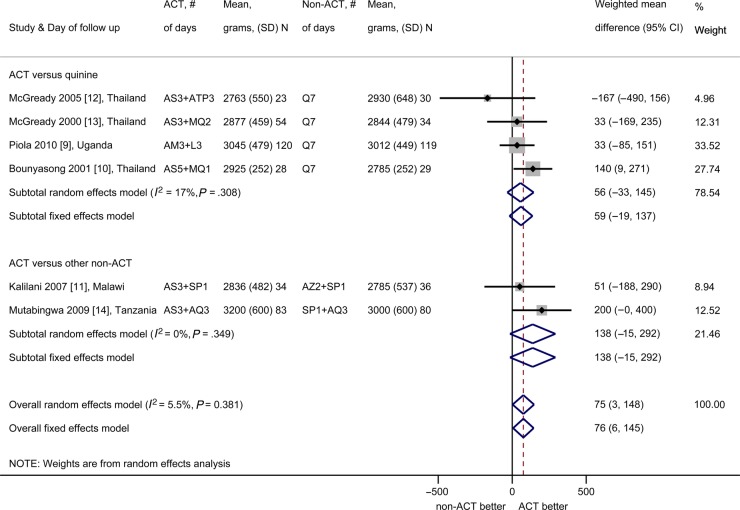
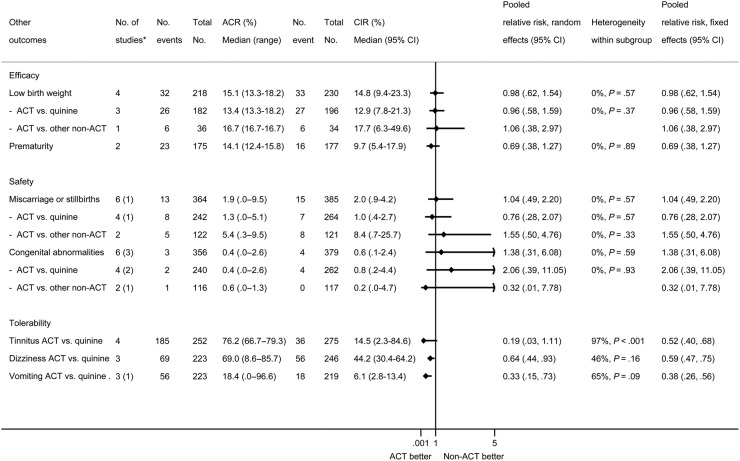
The World Health Organization recommends artemisinin-based combination therapies (ACTs) for the treatment of uncomplicated falciparum malaria in the second and third trimesters of pregnancy. We conducted a meta-analysis to compare efficacy, safety and tolerability of ACTs versus quinine and other non-ACT antimalarials. The median PCR-adjusted failure rate by days 28 to 63 in the non-ACT group was 6 (range 0-37) per 100 women, lower in the ACT group overall (pooled risk ratio [PRR] random effects, 0.41; 95% confidence interval [CI], 0.16-1.05; 6 trials), and significantly lower compared with oral quinine (PRR, 0.20; 95% CI, 0.08-0.49; 4 trials). There were no differences in fetal deaths and congenital abnormalities. Compared with quinine, artemisinin-based combinations therapies were associated with less tinnitus (PRR, 0.19; 95% CI, 0.03-1.11; 4 studies), dizziness (PRR, 0.64; 95% CI, 0.44-0.93; 3 trials), and vomiting (PRR, 0.33; 95% CI, 0.15-0.73; 3 trials). Artemisinin-based combination therapies are better than quinine in the second and third trimesters; their use should be encouraged among health workers.
Keywords: artemisinins; malaria; pregnancy; quinine; treatment.
Figures
References
-
- Desai M, ter Kuile FO, Nosten F et al. . Epidemiology and burden of malaria in pregnancy. Lancet Infect Dis 2007; 7:93–104. - PubMed
-
- World Health Organization. Guidelines for the Treatment of Malaria. Geneva: World Health Organization; 2006.
-
- World Health Organization. Guidelines for the Treatment of Malaria. 3rd ed Geneva: World Health Organization; 2015.
-
- World Health Organization. World Malaria Report 2014. Geneva: World Health Organization; 2014.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
