

Prevalence and Clinical Outcomes of Clostridium difficile Infection in the Intensive Care Unit: A Systematic Review and Meta-Analysis
- PMID: 26788544
- PMCID: PMC4716350
- DOI: 10.1093/ofid/ofv186
Prevalence and Clinical Outcomes of Clostridium difficile Infection in the Intensive Care Unit: A Systematic Review and Meta-Analysis
Abstract
Background. Intensive care unit (ICU) patients are at higher risk for Clostridium difficile infection (CDI).
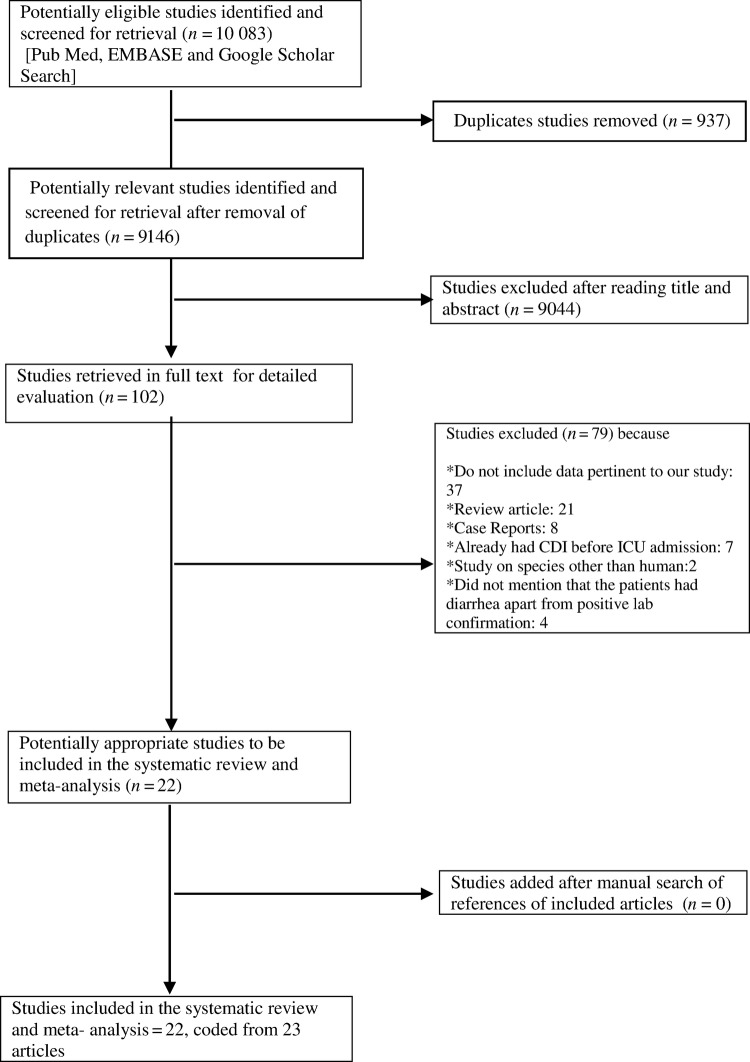
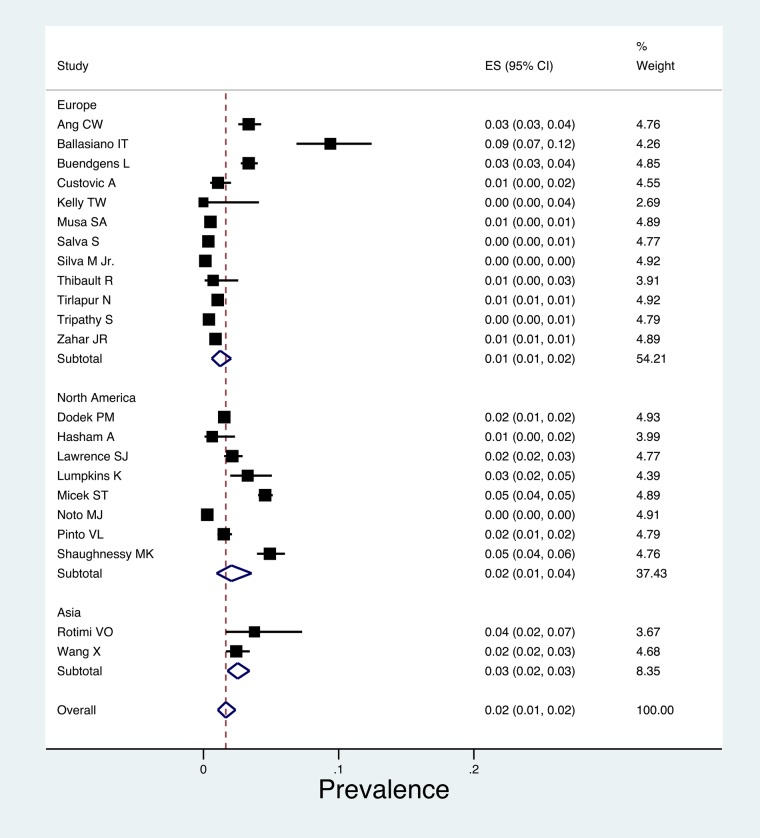
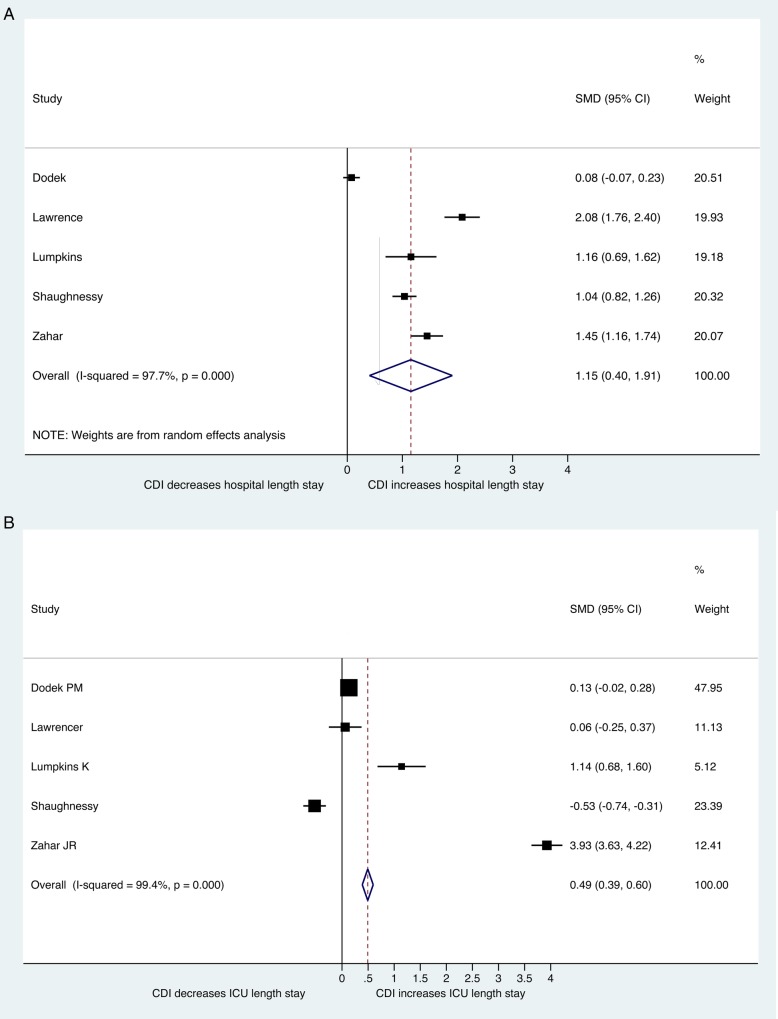
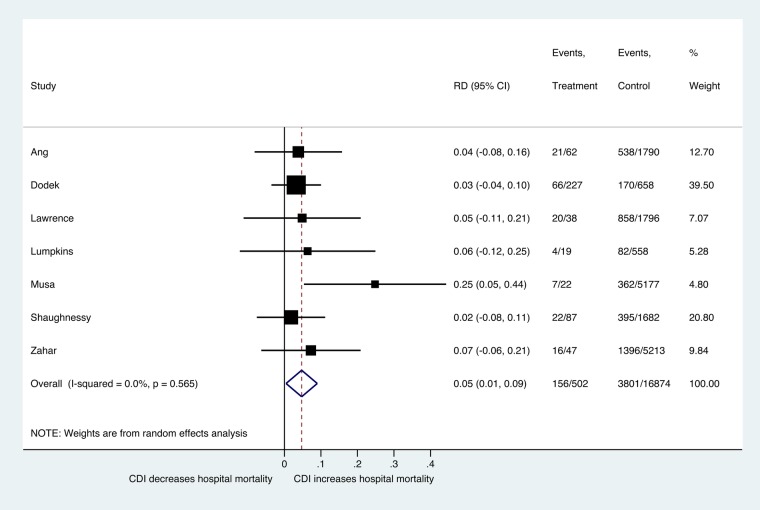
Methods: We performed a systematic review and meta-analysis of published studies from 1983 to 2015 using the PubMed, EMBASE, and Google Scholar databases to study the prevalence and outcomes of CDI in this patient population. Among the 9146 articles retrieved from the studies, 22 articles, which included a total of 80 835 ICU patients, were included in our final analysis. Results. The prevalence of CDI among ICU patients was 2% (95% confidence interval [CI], 1%-2%), and among diarrheic ICU patients the prevalence was 11% (95% CI, 6%-17%). Among CDI patients, 25% (95% CI, 5%-51%) were diagnosed with pseudomembranous colitis, and the estimated length of ICU stay before CDI acquisition was 10.74 days (95% CI, 5%-51%). The overall hospital mortality among ICU patients with CDI was 32% (95% CI, 26%-39%), compared with 24% (95% CI, 14%-36%) among those without CDI presenting a statistically significant difference in mortality risk (P = .030). It is worth noting that the length of ICU and hospital stay among CDI patients was significantly longer, compared with non-CDI patients (standardized mean of difference [SMD] = 0.49, 95% CI, .39%-.6%, P = .00 and SMD = 1.15, 95% CI, .44%-1.91%, P = .003, respectively). It is noteworthy that the morbidity score at ICU admission (Acute Physiology and Chronic Health Evaluation II [APACHE II]) was not statistically different between the 2 groups (P = .911), implying that the differences in outcomes can be attributed to CDI. Conclusions. The ICU setting is associated with higher prevalence of CDI. In this setting, CDI is associated with increased hospital mortality and prolonged ICU and overall hospital stay. These findings highlight the need for additional prevention and treatment studies in this setting.
Keywords: C difficile infection; ICU; length of stay; meta-analysis; mortality.
Figures
References
-
- Liolios A, Oropello JM, Benjamin E. Gastrointestinal complications in the intensive care unit. Clin Chest Med 1999; 20:329–45, viii. - PubMed
-
- Lucado J, Gould C, Elixhauser A. Clostridium difficile Infections (CDI) in Hospital Stays, 2009: Statistical Brief #124. Rockville, MD: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs, 2006. - PubMed
-
- Rowland SP, Dharmarajah B, Moore HM et al. Inferior vena cava filters for prevention of venous thromboembolism in obese patients undergoing bariatric surgery: a systematic review. Ann Surg 2015; 261:35–45. - PubMed
-
- Wells G, Shea B, O'Connell D et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed 1 December 2015.
LinkOut - more resources
Full Text Sources
Other Literature Sources
