

Violence-related periorbital trauma with a retained foreign body: a case report
- PMID: 26790751
- PMCID: PMC4721066
- DOI: 10.1186/s13256-015-0779-1
Violence-related periorbital trauma with a retained foreign body: a case report
Abstract
Background: Orbital fracture usually occurs as a result of blunt orbital and facial trauma and may involve ocular injuries. International studies on orbital floor fracture show several differences in epidemiology, diagnostic criteria, surgical treatment modalities, and complication rates; therefore, any comparison should be made with caution. Here we describe an unusual case involving a 19-year-old man with violence-related periorbital trauma, wherein a foreign body (a plastic pen cap) traversed the median wall of the maxillary sinus and penetrated the lower turbinate.
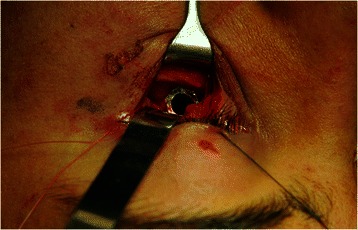
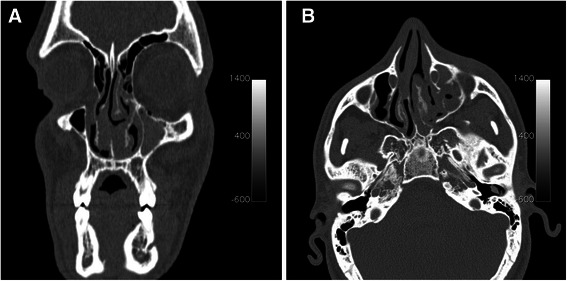
Case presentation: A 19-year-old Caucasian man was referred to our department with localized pain and swelling in the left suborbital region following a physical fight in May 2014. A clinical examination revealed no abnormalities in his eyeballs or eye movement, palpation of the orbital contour revealed no fractures, and ophthalmological evaluation showed no evidence of diplopia. A computed tomography scan revealed fractures in the left orbital floor, periorbital tissue herniation without muscular entrapment and left maxillary hemosinus were observed. A hypodense soft tissue mass was lodged in the left orbital floor, which extended to the median wall of the maxillary sinus and penetrated the left lower turbinate. Surgical exploration of the foreign body was conducted, revealing the foreign body to be a pen cap.
Conclusions: History or clinical examination alone may be inadequate to raise the suspicion of a retained periorbital foreign body in a situation of orbital region trauma. Computed tomography is important for the evaluation of periorbital injuries, especially because it could reveal the presence of a foreign body. Periorbital foreign bodies can be observed distinctly on computed tomography, which remains the most sensitive study and should be the first imaging modality in such cases.
Figures



References
-
- Exadaktylos AK, Sclabas GM, Smolka K, Rahal A, Andres RH, Zimmermann H, et al. The value of computed tomographic scanning in the diagnosis and management of orbital fractures associated with head trauma: a prospective, consecutive study at a level I trauma center. J Trauma. 2005;58:336–41. doi: 10.1097/01.TA.0000141874.73520.A6. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
