

A clinical role of staging laparoscopy in patients with radiographically defined locally advanced pancreatic ductal adenocarcinoma
- PMID: 26791083
- PMCID: PMC4721110
- DOI: 10.1186/s12957-016-0767-y
A clinical role of staging laparoscopy in patients with radiographically defined locally advanced pancreatic ductal adenocarcinoma
Abstract
Background: The aim of current study is to verify usefulness of staging laparoscopy (stag-lap) for patient's selection and to find prognostic factors in patients with radiographically defined locally advanced (RD-LA) pancreatic ductal adenocarcinoma (PDAC).
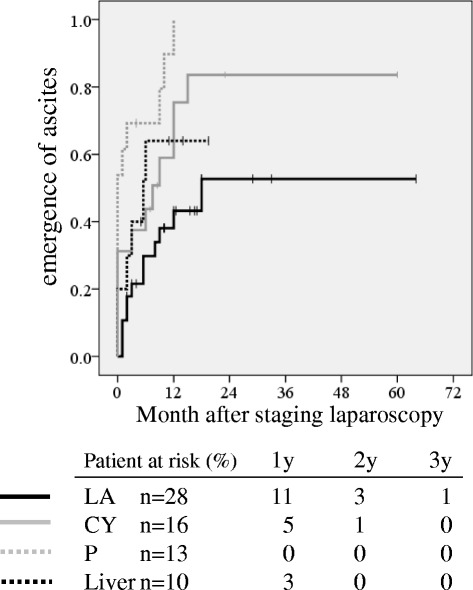
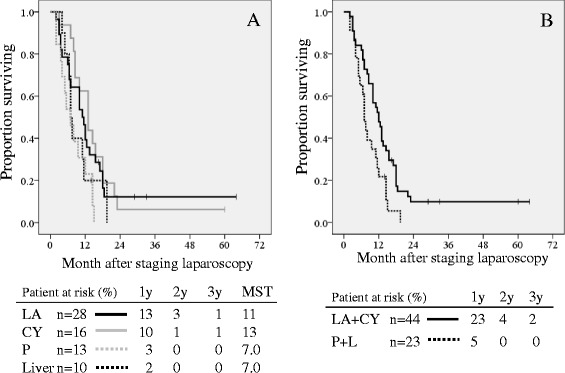
Methods: The LA disease was defined as an unresectable disease without distant organ metastasis based on resectability status of NCCN guideline in this study. Stag-lap was performed in 67 patients with RD-LA (2007-2012) which were divided into 4 groups according to metastatic site: group CY (peritoneal fluid or washing cytology positive and without any distant organ metastasis); group P (peritoneal dissemination); group L (liver metastasis); group LA (peritoneal fluid or washing cytology negative and without any distant organ metastasis). Clinical backgrounds, survival curves, and prognostic factors were investigated.
Results: There were 16 patients in CY group (24%), 13 patients in P group (19%), 10 patients in L group (15%), and 28 patients in LA group (42%). Median survival time was 13 months in CY group and 11 months in LA group, which was significantly better than 7 months in P group, respectively (p<0.05). The rate of emergence of ascites in LA was significantly better than in CY or P groups (p<0.05). Multivariate analysis showed that the presence of partial response and administration of second-line chemotherapy were significantly independent prognostic factors.
Conclusions: The majority of PDAC patients with RD-LA had occult distant organ metastasis. Clinical features and survival curves were different depending on the site of occult distant organ metastasis. Administration of second-line chemotherapy and responsiveness to chemotherapy were associated with favorable prognosis. Staging laparoscopy should be routinely performed in patients with RD-LA PDAC (UMIN000019936).
Figures
References
-
- Satoi S, Yamamoto H, Toyokawa H, Inoue K, Wada K, Yamamoto T, et al. Selective Use of staging laparoscopy based on Carbohydrate Antigen 19–9 level and tumor size in patients with radiographicallydefined potentially or borderline resectable pancreatic cancer. Pancreas. 2011;40:426–32. doi: 10.1097/MPA.0b013e3182056b1c. - DOI - PubMed
-
- Hori Y, SAGES Guidelines Committee. Diagnostic laparoscopy guidelines: This guideline was prepared by the SAGES Guidelines Committee and reviewed and approved by the Board of Governors of the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES), November 2007. Surg Endosc. 2008;22:1353-83. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
