

Predicting chemotherapeutic drug combinations through gene network profiling
- PMID: 26791325
- PMCID: PMC4726371
- DOI: 10.1038/srep18658
Predicting chemotherapeutic drug combinations through gene network profiling
Abstract
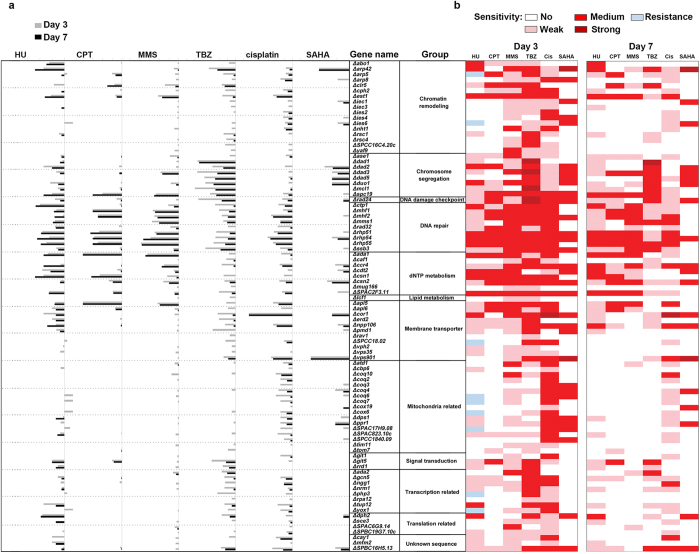
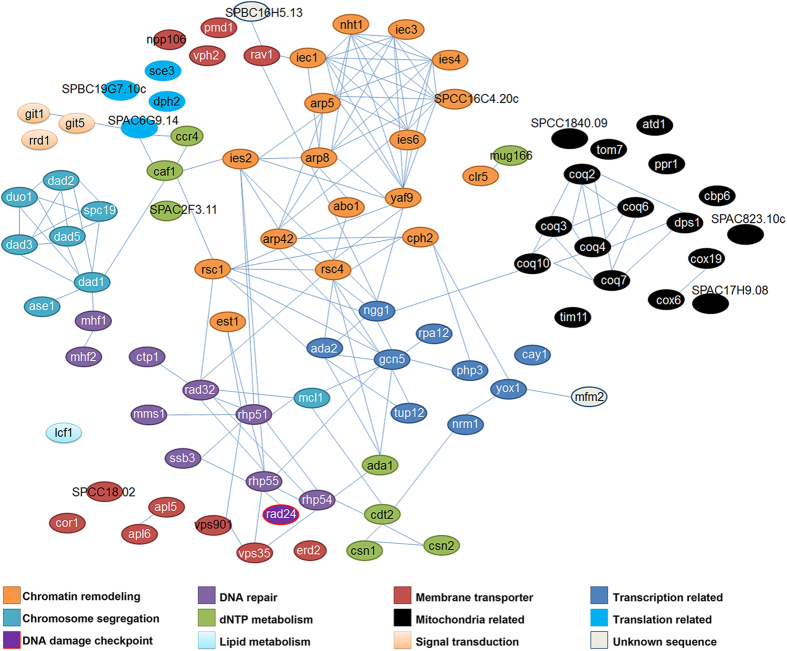
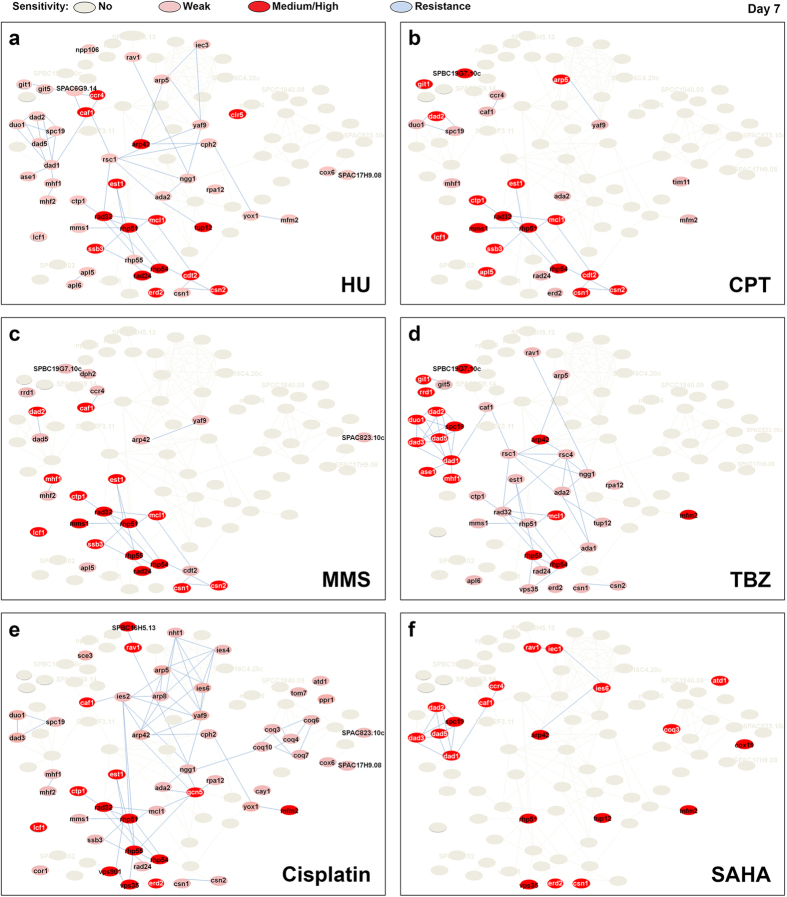
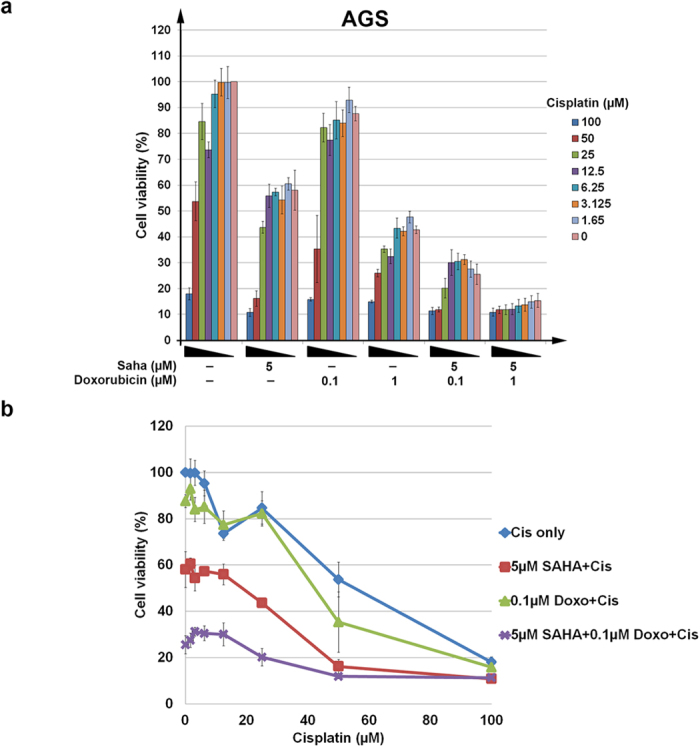
Contemporary chemotherapeutic treatments incorporate the use of several agents in combination. However, selecting the most appropriate drugs for such therapy is not necessarily an easy or straightforward task. Here, we describe a targeted approach that can facilitate the reliable selection of chemotherapeutic drug combinations through the interrogation of drug-resistance gene networks. Our method employed single-cell eukaryote fission yeast (Schizosaccharomyces pombe) as a model of proliferating cells to delineate a drug resistance gene network using a synthetic lethality workflow. Using the results of a previous unbiased screen, we assessed the genetic overlap of doxorubicin with six other drugs harboring varied mechanisms of action. Using this fission yeast model, drug-specific ontological sub-classifications were identified through the computation of relative hypersensitivities. We found that human gastric adenocarcinoma cells can be sensitized to doxorubicin by concomitant treatment with cisplatin, an intra-DNA strand crosslinking agent, and suberoylanilide hydroxamic acid, a histone deacetylase inhibitor. Our findings point to the utility of fission yeast as a model and the differential targeting of a conserved gene interaction network when screening for successful chemotherapeutic drug combinations for human cells.
Figures
Similar articles
-
Cellular robustness conferred by genetic crosstalk underlies resistance against chemotherapeutic drug doxorubicin in fission yeast.PLoS One. 2013;8(1):e55041. doi: 10.1371/journal.pone.0055041. Epub 2013 Jan 24. PLoS One. 2013. PMID: 23365689 Free PMC article.
-
Fitness profiling links topoisomerase II regulation of centromeric integrity to doxorubicin resistance in fission yeast.Sci Rep. 2015 Feb 11;5:8400. doi: 10.1038/srep08400. Sci Rep. 2015. PMID: 25669599 Free PMC article.
-
Histone deacetylase 1 gene expression and sensitization of multidrug-resistant neuroblastoma cell lines to cytotoxic agents by depsipeptide.J Natl Cancer Inst. 2007 Jul 18;99(14):1107-19. doi: 10.1093/jnci/djm044. Epub 2007 Jul 10. J Natl Cancer Inst. 2007. PMID: 17623797
-
Human B-cell cancer cell lines as a preclinical model for studies of drug effect in diffuse large B-cell lymphoma and multiple myeloma.Exp Hematol. 2014 Nov;42(11):927-38. doi: 10.1016/j.exphem.2014.07.263. Epub 2014 Jul 27. Exp Hematol. 2014. PMID: 25072621 Review.
-
Understanding the causes of multidrug resistance in cancer: a comparison of doxorubicin and sunitinib.Drug Resist Updat. 2009 Aug-Oct;12(4-5):114-26. doi: 10.1016/j.drup.2009.07.001. Epub 2009 Aug 3. Drug Resist Updat. 2009. PMID: 19648052 Review.
Cited by
-
Drug combinatorics and side effect estimation on the signed human drug-target network.BMC Syst Biol. 2016 Aug 15;10(1):74. doi: 10.1186/s12918-016-0326-8. BMC Syst Biol. 2016. PMID: 27526853 Free PMC article.
-
Resistance to Chemotherapeutic 5-Fluorouracil Conferred by Modulation of Heterochromatic Integrity through Ino80 Function in Fission Yeast.Int J Mol Sci. 2023 Jun 26;24(13):10687. doi: 10.3390/ijms241310687. Int J Mol Sci. 2023. PMID: 37445861 Free PMC article.
-
Understanding the molecular mechanisms of human diseases: the benefits of fission yeasts.Microb Cell. 2024 Aug 2;11:288-311. doi: 10.15698/mic2024.08.833. eCollection 2024. Microb Cell. 2024. PMID: 39104724 Free PMC article.
-
Cellular factories for coenzyme Q10 production.Microb Cell Fact. 2017 Mar 2;16(1):39. doi: 10.1186/s12934-017-0646-4. Microb Cell Fact. 2017. PMID: 28253886 Free PMC article. Review.
-
Optimizing drug combination and mechanism analysis based on risk pathway crosstalk in pan cancer.Sci Data. 2024 Jan 16;11(1):74. doi: 10.1038/s41597-024-02915-y. Sci Data. 2024. PMID: 38228620 Free PMC article.
References
-
- Fujita K. & Sasaki Y. Optimization of cancer chemotherapy on the basis of pharmacokinetics and pharmacodynamics: from patients enrolled in clinical trials to those in the ‘real world’. Drug Metab. Pharmacokinet. 29, 20–28 (2014). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
