

Usefulness of pT1 substaging in papillary urothelial bladder carcinoma
- PMID: 26791567
- PMCID: PMC4721190
- DOI: 10.1186/s13000-016-0466-6
Usefulness of pT1 substaging in papillary urothelial bladder carcinoma
Abstract
Background: When treating bladder cancer patients, the most significant problems usually concern cases with high-grade non-muscle-invasive carcinoma, and a better understanding of which patients would benefit from early radical cystectomy is urgently needed. The uropathology community is seeking more user-friendly approaches to distinguishing between T1 cancers exhibiting different types of clinical behavior.
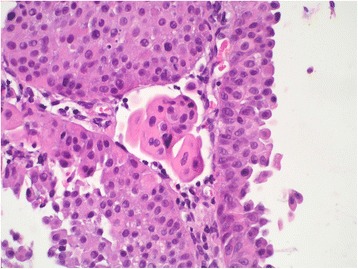
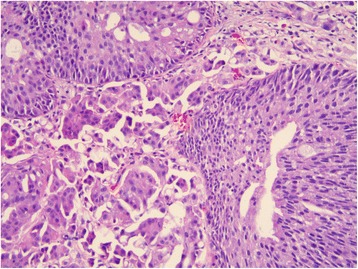
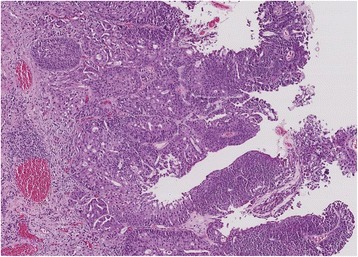
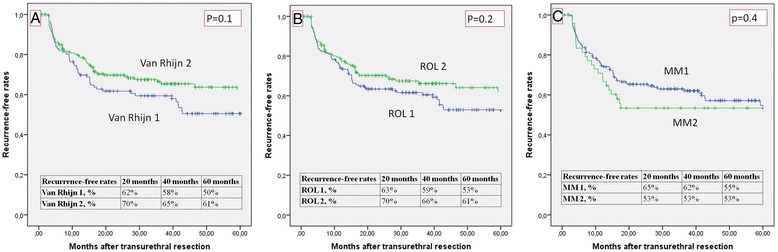
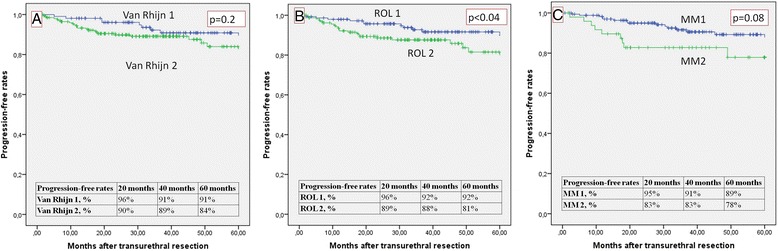
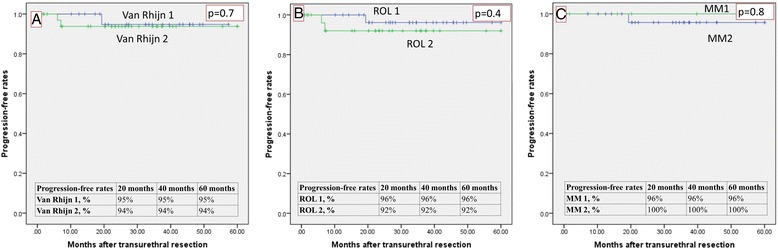
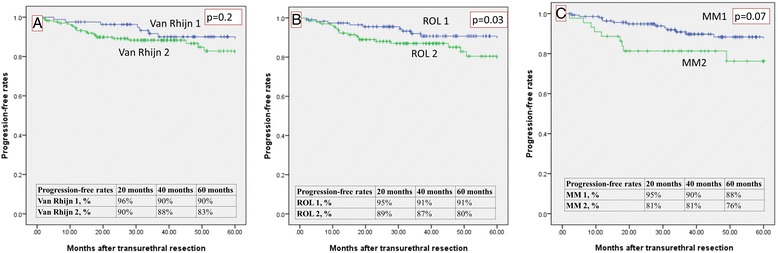
Methods: After a retrospective review, we selected a group of 314 patients who underwent transurethral resection of the bladder (TURB) and were diagnosed with high-grade urothelial carcinoma staged as T1. Three different substaging systems were applied: one was the anatomy-based T1 a/b; and two involved micrometric thresholds of either 0.5 mm of invasion (as proposed by van Rhijn et al.), or 1 mm of invasion (as proposed in the present study). Early reTUR (repeated transurethral resection) was performed in 250 patients, and the same substaging approaches were applied to cases of T1.
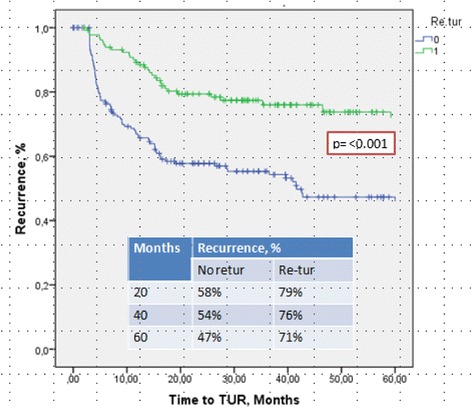
Results: It proved feasible to apply the 1 mm substaging system in 100 % of cases, the van Rhijn system in 100 %, and the anatomy-based method (T1 a/b) in 72.3 % of cases. At a mean follow-up of 46 months, the recurrence-free survival rate was significantly better (p < 0.001) in the group that underwent reTUR, while none of the three substaging systems reliably predicted recurrences. The 1 mm did seem promising, however, as a threshold for predicting progression, reaching statistical significance in the Kaplan Meier estimates (p < 0.04).
Conclusion: Our study shows that micrometric substaging is feasible in this setting and should be extended to include any early reTUR to complete the substaging done after the first TURB. It can also provide helpful prognostic information.
Figures
Comment in
-
Re: Usefulness of pT1 Substaging in Papillary Urothelial Bladder Carcinoma.J Urol. 2016 Sep;196(3):689. doi: 10.1016/j.juro.2016.06.036. Epub 2016 Jun 15. J Urol. 2016. PMID: 27597063 No abstract available.
References
-
- WHO Classification of Tumours . In: Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs. John E, Guido S, Jonathan E, Sesterhenn IA, editors. Lyon: IARC Press; 2004.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
