

Review
doi: 10.1038/nature17038.
Metastatic colonization by circulating tumour cells
Affiliations
- PMID: 26791720
- PMCID: PMC5029466
- DOI: 10.1038/nature17038
Item in Clipboard
Review
Metastatic colonization by circulating tumour cells
Nature.
.
Abstract
Metastasis is the main cause of death in people with cancer. To colonize distant organs, circulating tumour cells must overcome many obstacles through mechanisms that we are only now starting to understand. These include infiltrating distant tissue, evading immune defences, adapting to supportive niches, surviving as latent tumour-initiating seeds and eventually breaking out to replace the host tissue. They make metastasis a highly inefficient process. However, once metastases have been established, current treatments frequently fail to provide durable responses. An improved understanding of the mechanistic determinants of such colonization is needed to better prevent and treat metastatic cancer.
Figures
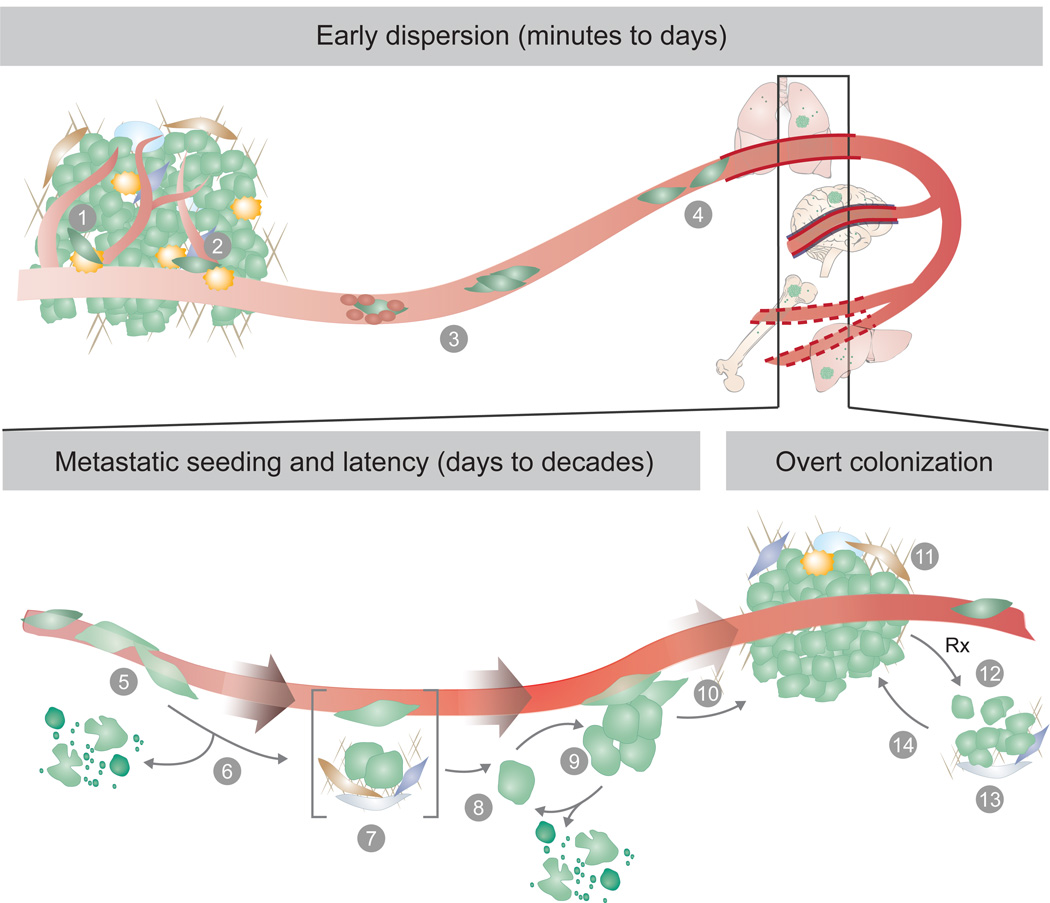
Metastasis proceeds through multiple steps and restrictive bottlenecks. Factors including the germline, tumour cell of origin, cancer cell plasticity, host tissue stroma, and response to therapy may influence the emergence of metastatic traits, and the probability that a cancer cell will complete all the steps towards overt metastasis. The pre-colonization phase of metastasis involves a series of events that cancer cells go through in a time scale of minutes to hours, including: (1) local invasion of cancer cells in the primary tumour, (2) intravasation into the tumour vasculature, (3) circulation of cancer cells as single cells or cell clusters, coated with platelets, (4) arrest in capillaries at the distant site and, (5) extravasation into the parenchyma of target organs for metastatic colonization. Colonization can be parsed into many steps that occur in a time scale of years. After extravasation, metastatic colonization comprises (6) resistance to immunity and other host tissue defences, (7) settlement in supportive niches for survival and retention of stem-like tumour-initiating capacity, (8) entry into latency as single cells, or (9) as indolent micrometastases. During the latency phase, which can last from months to decades, disseminated cancer cells must achieve long-term survival and may acquire traits for the eventually overtaking of the host tissue. The disseminated cancer cells may then break out of latency, reinitiating overt outgrowth (10), and overtaking the local tissue microenvironment (11). Once metastases become clinically manifest, therapeutic treatment may partially eliminate the tumour (12). However, under therapy-induced stress, cancer cells and non-neoplastic stromal cells mobilize survival signals (13) that nurse the residual disease until minority drug-resistant clones emerge and lead the outgrowth of a drug-resistant tumour (14). Different host tissue microenvironments select for cancer cells with distinct metastatic traits, giving rise to organ-specific metastatic cell populations.
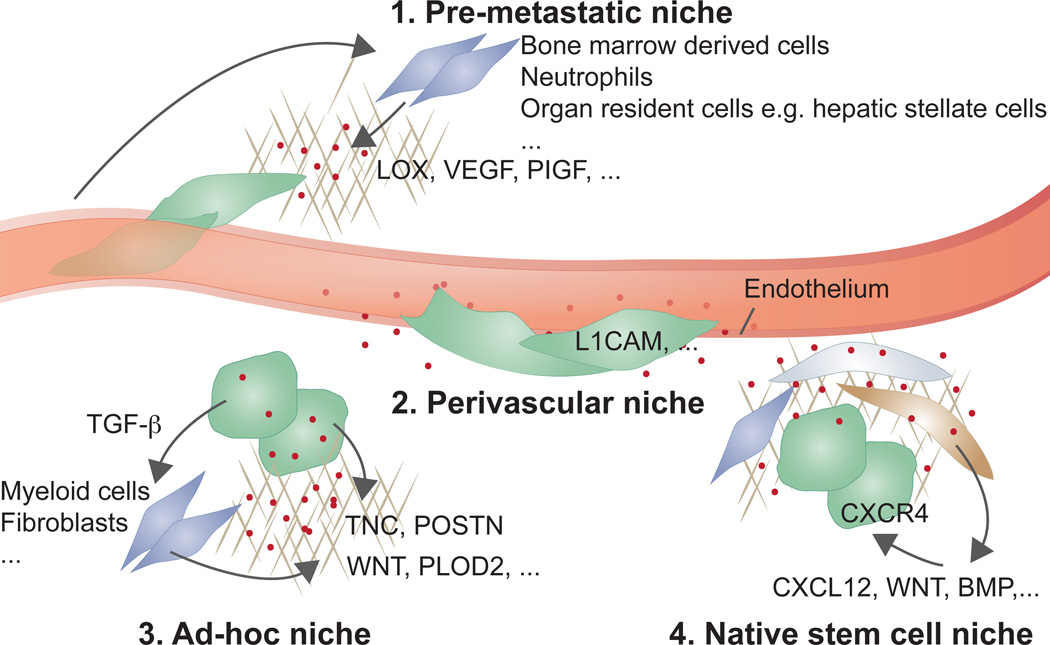
Cancer cells that infiltrate distant tissues survive and retain stem cell potential by situating in supportive niches, akin to the niches that support normal adult stem cells. Different niches have been proposed: (1) pre-metastatic niches formed by systemic signals from the primary tumour that recruit supportive stromal cells before the arrival of cancer cells from the tumour; (2) perivascular niches for cancer cells that spread over the capillary basement membrane right after extravasation, remaining in close apposition to endothelial cells and their paracrine factors; (3) ad-hoc niches constituted by secretory products from the cancer cells themselves that act in an autocrine manner or recruit stromal components as sources of supportive signals; and (4), native stem cell niches of the host tissue, which are invaded by the infiltrated cancer cells to directly occupy a supportive microenvironment. The four entities may be partly overlapping in location or composition. For example, native stem cell niches could be perivascular, or pre-metastatic signals might combine with ad-hoc niches.
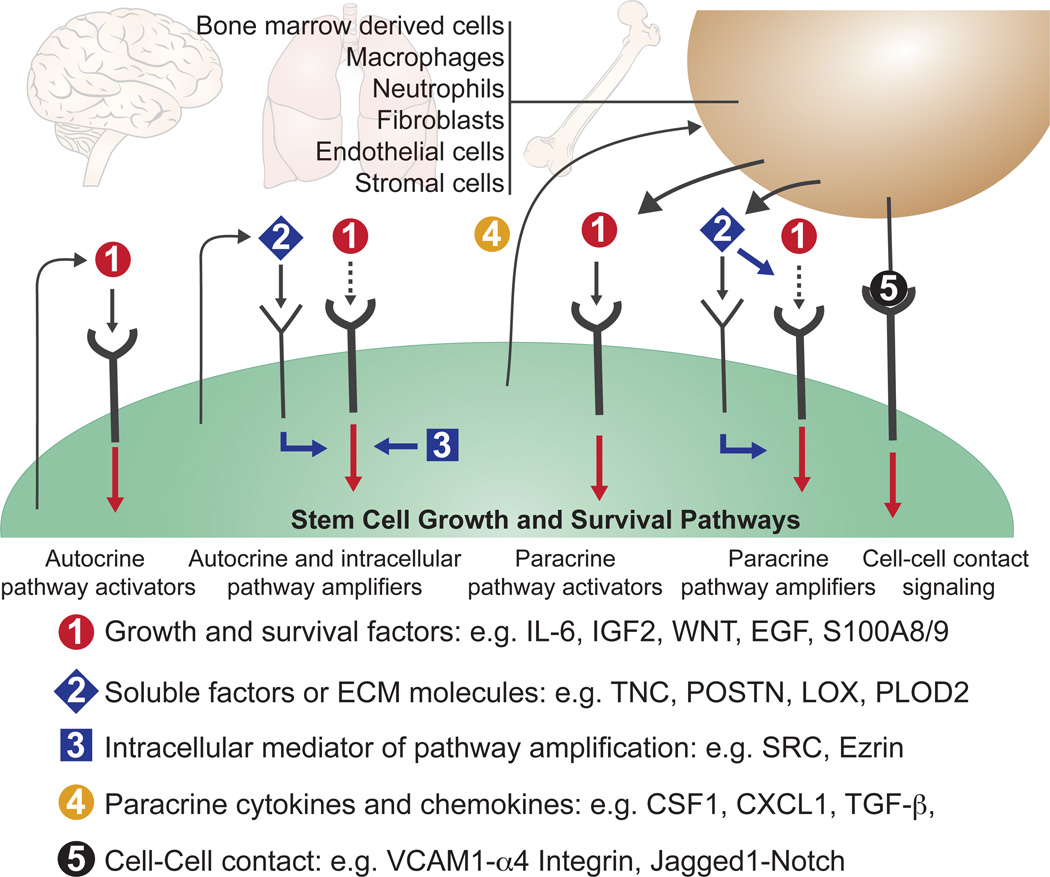
During one or more stages of the metastatic colonization process, metastasis-initiating cells require the activity of a common set of pathways that support the growth and survival of stem and progenitor cells. After infiltrating distant tissues that offer limiting levels of pathway activators, the disseminated cancer cells secure pathway activation through autocrine or paracrine mediators that directly activate these pathways (1), or amplify the responsiveness of the pathways to low levels of stromal activators (2, 3). Cancer cells may express autocrine (1, 2) and intracellular (3) pathway activators and amplifiers. Cancer cells may also express paracrine factors (4) that recruit stromal cells as sources of soluble activators and amplifiers, or may achieve pathway activation through direct cell-cell contact. Specific examples of these various mediators are listed in the figure and discussed in the text.
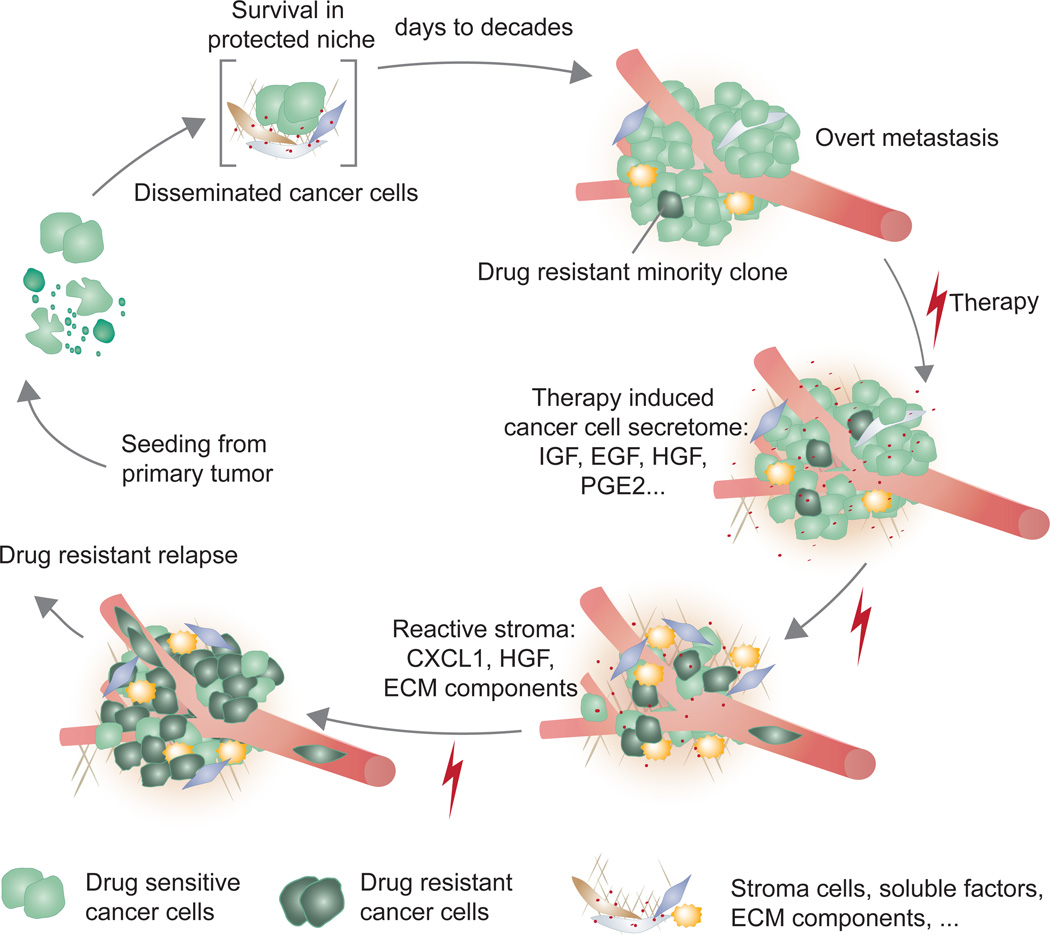
Latent metastasis results from conditions that preserve the survival and tumour-initiating ability of disseminated cancer cells. Eliminating latent metastasis by targeting these survival mechanisms would prevent metastasis. Once cancer cells break out of the latency state and form manifest metastasis, the condition is treated with combinations of conventional chemotherapy, targeted therapy, and/or immunotherapy. The treatment may dramatically reduce the metastatic burden, but tumour elimination is frequently incomplete. Significant segments of the tumour cell population withstand treatment by adaptation of their intracellular pathways or activation of supportive paracrine inputs. Under the stress of targeted therapy, drug-sensitive cancer cells express a large number of secreted factors (therapy-induced secretome) that salvage drug-sensitive cells and accelerate the growth of minority drug-resistant clones. The accelerated growth leads drug-resistant clones to drive relapse as a drug-resistant tumour. The growth and survival mechanisms utilized by residual cancer cells under treatment might resemble those utilized by their predecessors during the latent phase before overt colonization in this model.
References
-
- Braun S, et al. A pooled analysis of bone marrow micrometastasis in breast cancer. N Engl J Med. 2005;353:793–802. - PubMed
-
- Wong CW, et al. Apoptosis: an early event in metastatic inefficiency. Cancer Res. 2001;61:333–338. - PubMed
-
- Chambers AF, Groom AC, MacDonald IC. Dissemination and growth of cancer cells in metastatic sites. Nat Rev Cancer. 2002;2:563–572. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
