

The Nitrate-Nitrite-NO Pathway and Its Implications for Heart Failure and Preserved Ejection Fraction
- PMID: 26792295
- PMCID: PMC4755323
- DOI: 10.1007/s11897-016-0277-9
The Nitrate-Nitrite-NO Pathway and Its Implications for Heart Failure and Preserved Ejection Fraction
Abstract
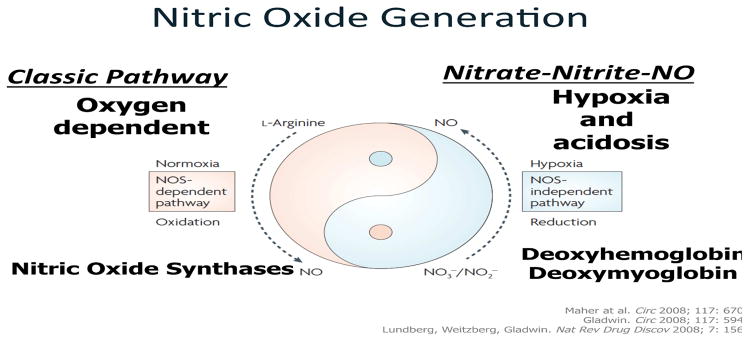
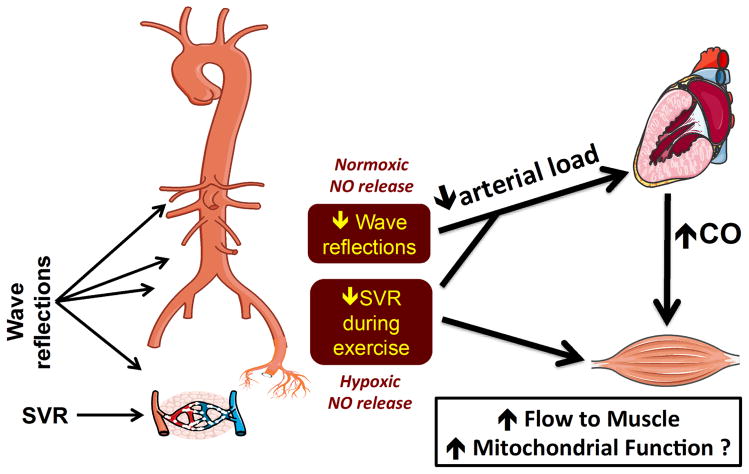
The pathogenesis of exercise intolerance in patients with heart failure and preserved ejection fraction (HFpEF) is likely multifactorial. In addition to cardiac abnormalities (diastolic dysfunction, abnormal contractile reserve, chronotropic incompetence), several peripheral abnormalities are likely to be involved. These include abnormal pulsatile hemodynamics, abnormal arterial vasodilatory responses to exercise, and abnormal peripheral O2 delivery, extraction, and utilization. The nitrate-nitrite-NO pathway is emerging as a potential target to modify key physiologic abnormalities, including late systolic left ventricular (LV) load from arterial wave reflections (which has deleterious short- and long-term consequences for the LV), arterial vasodilatory reserve, muscle O2 delivery, and skeletal muscle mitochondrial function. In a recently completed randomized trial, the administration of a single dose of exogenous inorganic nitrate has been shown to exert various salutary arterial hemodynamic effects, ultimately leading to enhanced aerobic capacity in patients with HFpEF. These effects have the potential for both immediate improvements in exercise tolerance and for long-term "disease-modifying" effects. In this review, we provide an overview of key mechanistic contributors to exercise intolerance in HFpEF, and of the potential therapeutic role of drugs that target the nitrate-nitrite-NO pathway.
Keywords: Afterload; Heart failure with preserved ejection fraction; Inorganic nitrate; Mitochondria; Therapy; Wave reflections.
Conflict of interest statement
Conflict of Interest
Julio A. Chirinos has received personal fees from Brystol Myers Squibb, OPKO Healthcare, Fukuda Denshi, Microsoft and Merck, grants from National Institutes of Health, American College of Radiology Network, Fukuda Denshi, Microsoft, Brystol Myers Squibb, and non-financial support from Atcor Medical outside the submitted work. In addition, Dr. Chirinos is named as inventor in a pending University of Pennsylvania patent application for the use of inorganic nitrates/nitrites for the treatment of HFpEF.
Payman Zamani declares that he has no conflict of interest.
Figures
References
-
- Vasan RS, Benjamin EJ, Levy D. Prevalence, clinical features and prognosis of diastolic heart failure: an epidemiologic perspective. Journal of the American College of Cardiology. 1995;26:1565–74. - PubMed
-
- Redfield MM, Jacobsen SJ, Burnett JC, Jr, Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: appreciating the scope of the heart failure epidemic. JAMA : the journal of the American Medical Association. 2003;289:194–202. - PubMed
-
- Kitzman DW, Gardin JM, Gottdiener JS, Arnold A, Boineau R, Aurigemma G, Marino EK, Lyles M, Cushman M, Enright PL. Importance of heart failure with preserved systolic function in patients > or = 65 years of age. CHS Research Group. Cardiovascular Health Study. The American journal of cardiology. 2001;87:413–9. - PubMed
-
- Devereux RB, Roman MJ, Liu JE, Welty TK, Lee ET, Rodeheffer R, Fabsitz RR, Howard BV. Congestive heart failure despite normal left ventricular systolic function in a population-based sample: the Strong Heart Study. The American journal of cardiology. 2000;86:1090–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
