

Presumptive Late-Onset Ankylosing Spondylitis Simulating Osteoblastic Skeletal Metastasis in a Patient With a History of Prostate Carcinoma: A Diagnostic Challenge
- PMID: 26793037
- PMCID: PMC4688560
- DOI: 10.1016/j.jcm.2015.06.005
Presumptive Late-Onset Ankylosing Spondylitis Simulating Osteoblastic Skeletal Metastasis in a Patient With a History of Prostate Carcinoma: A Diagnostic Challenge
Abstract
Objective: The purpose of this report is to present a presumptive case of ankylosing spondylitis with late stage progression that simulated osteoblastic metastasis in a patient with a history of prostate carcinoma.
Clinical features: A 67-year-old white man presented to a chiropractic clinic complaining of severe and worsening acute low back pain and right foot "numbness." Further questioning also revealed a history of prostate carcinoma.
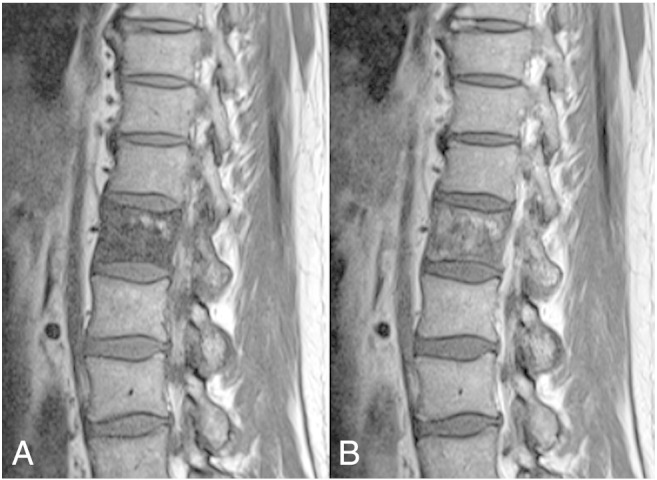
Intervention and outcome: Imaging examination revealed a sclerotic pedicle and increased uptake of radiopharmaceutical on a nuclear medicine bone scan highly suggestive of osteoblastic skeletal metastasis. Further evaluation, however, revealed that the bone sclerosis was not the result of skeletal metastasis, but more consistent with a seronegative spondyloarthritis such as ankylosing spondylitis.
Conclusion: This report describes a presumptive case of ankylosing spondylitis simulating skeletal metastasis in a patient with a past medical history of prostate cancer. This atypical presentation illustrates the inherent uncertainty of diagnosis and how that uncertainty can be challenging in clinical practice. It also reinforces that it is critical for healthcare providers to consider a wide spectrum of differential diagnoses to avoid misdiagnoses and inappropriate interventions.
Keywords: Ankylosing spondylitis; Chiropractic; Diagnosis; Neoplasm metastasis; Spondylarthritis.
Figures




Similar articles
-
Reply to "Presumptive Late-Onset Ankylosing Spondylitis Simulating Osteoblastic Skeletal Metastasis in a Patient With a History of Prostate Carcinoma: A Diagnostic Challenge".J Chiropr Med. 2017 Jun;16(2):180-181. doi: 10.1016/j.jcm.2017.01.004. Epub 2017 Mar 10. J Chiropr Med. 2017. PMID: 28559760 Free PMC article. No abstract available.
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Differential diagnosis and management of ankylosing spondylitis masked as adhesive capsulitis: a resident's case problem.J Orthop Sports Phys Ther. 2012 Oct;42(10):842-52. doi: 10.2519/jospt.2012.4050. Epub 2012 Jul 26. J Orthop Sports Phys Ther. 2012. PMID: 22836244
-
Abdominal aortitis in HLA-B27+ spondyloarthritis: case report with 5-year follow-up and literature review.Semin Arthritis Rheum. 2014 Dec;44(3):305-8. doi: 10.1016/j.semarthrit.2014.05.012. Epub 2014 May 15. Semin Arthritis Rheum. 2014. PMID: 24935530 Review.
-
[Ankylosed spine fractures with spondylitis or diffuse idiopathic skeletal hyperostosis: diagnosis and complications].Rev Chir Orthop Reparatrice Appar Mot. 2004 Sep;90(5):456-65. doi: 10.1016/s0035-1040(04)70173-7. Rev Chir Orthop Reparatrice Appar Mot. 2004. PMID: 15502769 Review. French.
Cited by
-
Reply to "Presumptive Late-Onset Ankylosing Spondylitis Simulating Osteoblastic Skeletal Metastasis in a Patient With a History of Prostate Carcinoma: A Diagnostic Challenge".J Chiropr Med. 2017 Jun;16(2):180-181. doi: 10.1016/j.jcm.2017.01.004. Epub 2017 Mar 10. J Chiropr Med. 2017. PMID: 28559760 Free PMC article. No abstract available.
References
-
- Olivieri I., Salvarani C., Cantini F., Ciancio G., Padula A. Ankylosing spondylitis and undifferentiated spondyloarthropathies: a clinical review and description of a disease subset with older age at onset. Curr Opin Rheumatol. 2001;13(4):280–284. - PubMed
-
- Raychaudhuri S.P., Atul D. The classification and diagnostic criteria of ankylosing spondylitis. J Autoimmun. 2014;48:128–133. - PubMed
-
- Khan M.A. Update on spondyloarthropathies. Ann Intern Med. 2002;136(12):896–907. - PubMed
-
- Sampaio-Barros P.D., Bertolo M.B., Kraemer M.H., Neto J.F., Samara A.M. Ankylosing spondylitis: patterns of disease in a Brazilian population of 147 patients. J Rheumatol. 2001;28(3):560–565. - PubMed
-
- Toussirot É., Wendling D. Late-Onset Ankylosing Spondylitis and Related Spondylarthropathies. Drugs Aging. 2005;22(6):451–469. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
