

Meta-analysis of the efficacy and safety of adding an angiotensin receptor blocker (ARB) to a calcium channel blocker (CCB) following ineffective CCB monotherapy
- PMID: 26793346
- PMCID: PMC4703641
- DOI: 10.3978/j.issn.2072-1439.2015.12.39
Meta-analysis of the efficacy and safety of adding an angiotensin receptor blocker (ARB) to a calcium channel blocker (CCB) following ineffective CCB monotherapy
Abstract
Background: We conducted this meta-analysis to systematically review and analyze the clinical benefits of angiotensin receptor blocker (ARB) combined with calcium channel blocker (CCB) following ineffective CCB monotherapy.
Methods: PubMed was searched for articles published until August 2015. Randomized controlled trials (RCTs) evaluating the clinical benefits of ARB combined with CCB following ineffective CCB monotherapy were included. The primary efficacy endpoint of the studies was normal rate of blood pressure, the secondary efficacy endpoints were the response rate and change in blood pressure from baseline. The safety endpoint of the studies was incidence of adverse events. Differences are expressed as relative risks (RRs) with 95% confidence intervals (CIs) for dichotomous outcomes and weighted mean differences (WMDs) with 95% CIs for continuous outcomes. Heterogeneity across studies was tested by using the I(2) statistic.
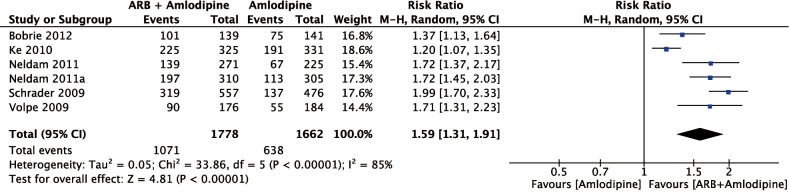
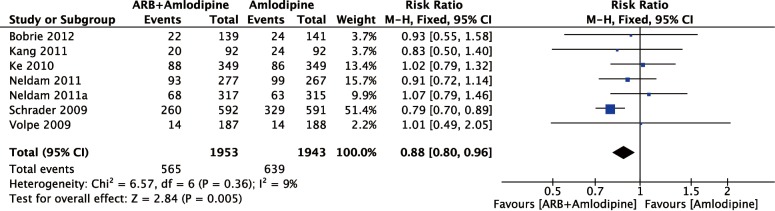
Results: Seven RCTs were included and had sample sizes ranging from 185 to 1,183 subjects (total: 3,909 subjects). The pooled analysis showed that the on-target rate of hypertension treatment was significantly higher in the amlodipine + ARB group than in the amlodipine monotherapy group (RR =1.59; 95% CI, 1.31-1.91; P<0.01). The response rate of systolic blood pressure (SBP) (RR =1.28; 95% CI, 1.04-1.58; P<0.01) and diastolic blood pressure (DBP) (RR =1.27; 95% CI, 1.12-1.44; P=0.04) were significantly higher in the amlodipine + ARB group than in the amlodipine monotherapy group. The change in SBP (RR =-3.56; 95% CI, -7.76-0.63; P=0.10) and DBP (RR =-3.03; 95% CI, -6.51-0.45; P=0.09) were higher in hypertensive patients receiving amlodipine + ARB but the difference did not reach statistical significance. ARB + amlodipine treatment carried a lower risk of adverse events relative to amlodipine monotherapy (RR =0.88; 95% CI, 0.80-0.96; P<0.01).
Conclusions: The results of our meta-analysis demonstrate that adding an ARB to CCB after initial ineffective CCB monotherapy, significantly improved blood pressure control and the percentage of on-target hypertension treatment with significantly reduced incidence of adverse events compared with continued CCB monotherapy.
Keywords: Hypertension; angiotensin receptor antagonists; calcium channel blockers (CCB); drug combinations; meta-analysis.
Conflict of interest statement
Figures



References
-
- Lawes CM, Vander Hoorn S, Rodgers A, et al. Global burden of blood-pressure-related disease, 2001. Lancet 2008;371:1513-8. - PubMed
-
- Kannel WB. Elevated systolic blood pressure as a cardiovascular risk factor. Am J Cardiol 2000;85:251-5. - PubMed
-
- Kannel WB. Historic perspectives on the relative contributions of diastolic and systolic blood pressure elevation to cardiovascular risk profile. Am Heart J 1999;138:205-10. - PubMed
-
- Yu JM, Kong QY, Schoenhagen P, et al. The prognostic value of long-term visit-to-visit blood pressure variability on stroke in real-world practice: a dynamic cohort study in a large representative sample of Chinese hypertensive population. Int J Cardiol 2014;177:995-1000. - PubMed
-
- Turnbull F, Blood Pressure Lowering Treatment Trialists' Collaboration . Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trials. Lancet 2003;362:1527-35. - PubMed
LinkOut - more resources
Full Text Sources