

Pharmacokinetics and Safety of Elotuzumab Combined With Lenalidomide and Dexamethasone in Patients With Multiple Myeloma and Various Levels of Renal Impairment: Results of a Phase Ib Study
- PMID: 26795075
- PMCID: PMC6857171
- DOI: 10.1016/j.clml.2015.12.007
Pharmacokinetics and Safety of Elotuzumab Combined With Lenalidomide and Dexamethasone in Patients With Multiple Myeloma and Various Levels of Renal Impairment: Results of a Phase Ib Study
Abstract
Introduction: The present study evaluated the pharmacokinetics and safety of elotuzumab, a humanized IgG1 monoclonal antibody against signaling lymphocyte activation molecule-F7, combined with lenalidomide and dexamethasone, in patients with multiple myeloma (MM) and renal impairment.
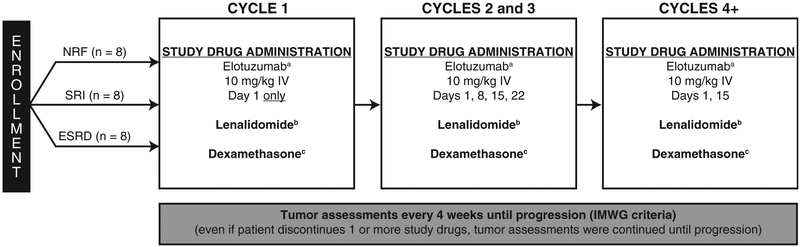
Patients and methods: Patients with MM and normal renal function (NRF) (creatinine clearance [CrCl] ≥ 90 mL/min), severe renal impairment (SRI) (CrCl < 30 mL/min, not requiring dialysis), or end-stage renal disease (ESRD) (requiring dialysis) were enrolled in this open-label, phase Ib study. Elotuzumab (10 mg/kg), lenalidomide (5-25 mg), and dexamethasone (40 mg) were administered in 28-day cycles until disease progression or unacceptable toxicity developed. The primary endpoint was single-dose elotuzumab pharmacokinetics.
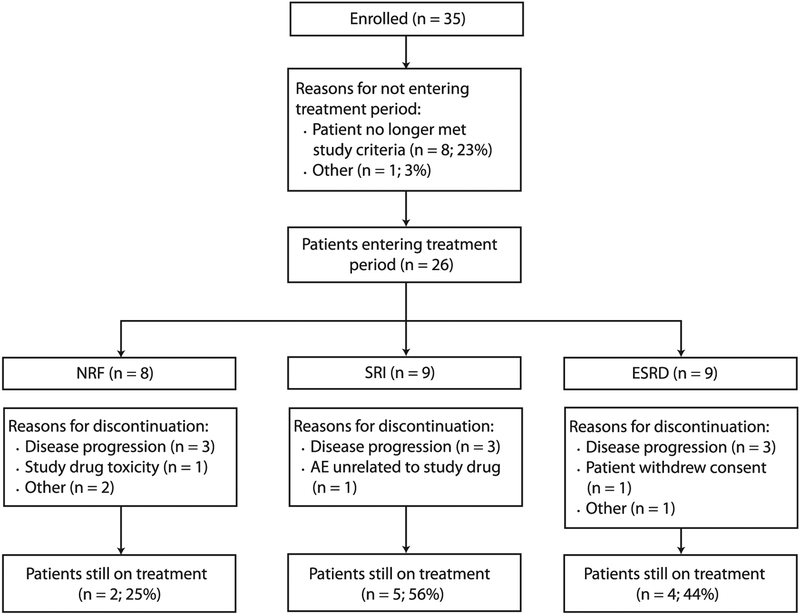
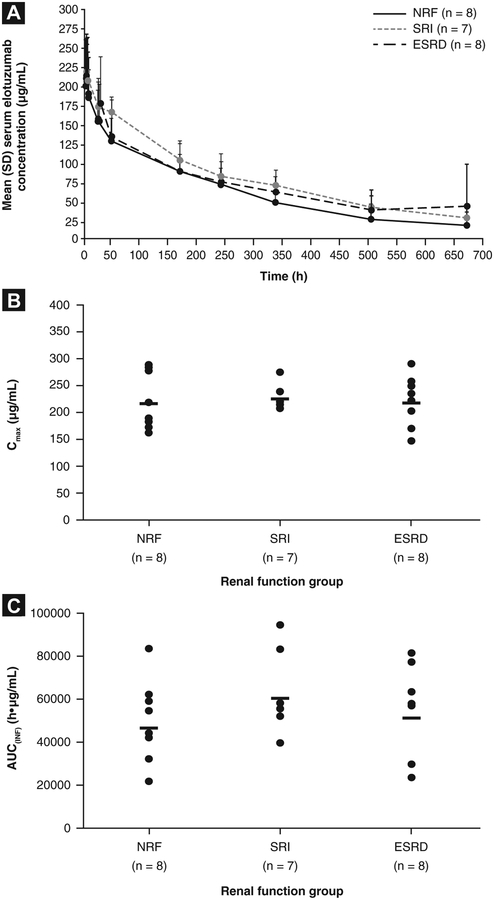
Results: A total of 26 patients (median age, 63 years) were treated (NRF, n = 8; SRI, n = 9; ESRD, n = 9). The median baseline CrCl was 105 mL/min (range, 84-146 mL/min) for those with NRF and 26 mL/min (range, 15-33 mL/min) for those with SRI. Twenty-three patients (89%) had received previous therapy (median, 2 regimens; range, 1-7). Treatment was discontinued in 6 patients with NRF, 4 with SRI, and 5 with ESRD, primarily because of disease progression. The mean elotuzumab serum concentrations were comparable across groups (n = 23). No statistically significant differences were observed in the maximum observed serum concentration, area under the concentration-time curve from time 0 to the last quantifiable serum concentration, or area under the concentration-time curve from time 0 to infinity when the SRI and ESRD groups were compared with the NRF group (P > .05). All patients had ≥ 1 adverse event (AE). Of the 8 patients with NRF, 9 with SRI, and 9 with ESRD, 7, 8, and 7 experienced grade 3 to 4 AEs. The overall response rates were 75% in the NRF, 67% in the SRI, and 56% in the ESRD groups.
Conclusion: The results of the present study support the use of elotuzumab for the treatment of patients with MM and renal dysfunction without dose adjustment.
Keywords: Creatinine clearance; End-stage renal disease; Glomerular filtration rate; Monoclonal antibody; SLAMF7.
Copyright © 2016 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Clark AD, Shetty A, Soutar R Renal failure and multiple myeloma: pathogenesis and treatment of renal failure and management of underlying myeloma. Blood Rev 1999; 13:79–90. - PubMed
-
- Blade J, Fernandez-Llama P, Bosch F, et al. Renal failure in multiple myeloma: presenting features and predictors of outcome in 94 patients from a single institution. Arch Intern Med 1998; 158:1889–93. - PubMed
-
- Leung N, Behrens J. Current approach to diagnosis and management of acute renal failure in myeloma patients. Adv Chronic Kidney Dis 2012; 19:297–302. - PubMed
-
- San-Miguel JF, Richardson PG, Sonneveld P, et al. Efficacy and safety of bortezomib in patients with renal impairment: results from the APEX phase 3 study. Leukemia 2008; 22:842–9. - PubMed
-
- Eleutherakis-Papaiakovou V, Bamias A, Gika D, et al. Renal failure in multiple myeloma: incidence, correlations, and prognostic significance. Leuk Lymphoma 2007; 48:337–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
