

BMPR2 mutations and survival in pulmonary arterial hypertension: an individual participant data meta-analysis
- PMID: 26795434
- PMCID: PMC4737700
- DOI: 10.1016/S2213-2600(15)00544-5
BMPR2 mutations and survival in pulmonary arterial hypertension: an individual participant data meta-analysis
Abstract
Background: Mutations in the gene encoding the bone morphogenetic protein receptor type II (BMPR2) are the commonest genetic cause of pulmonary arterial hypertension (PAH). However, the effect of BMPR2 mutations on clinical phenotype and outcomes remains uncertain.
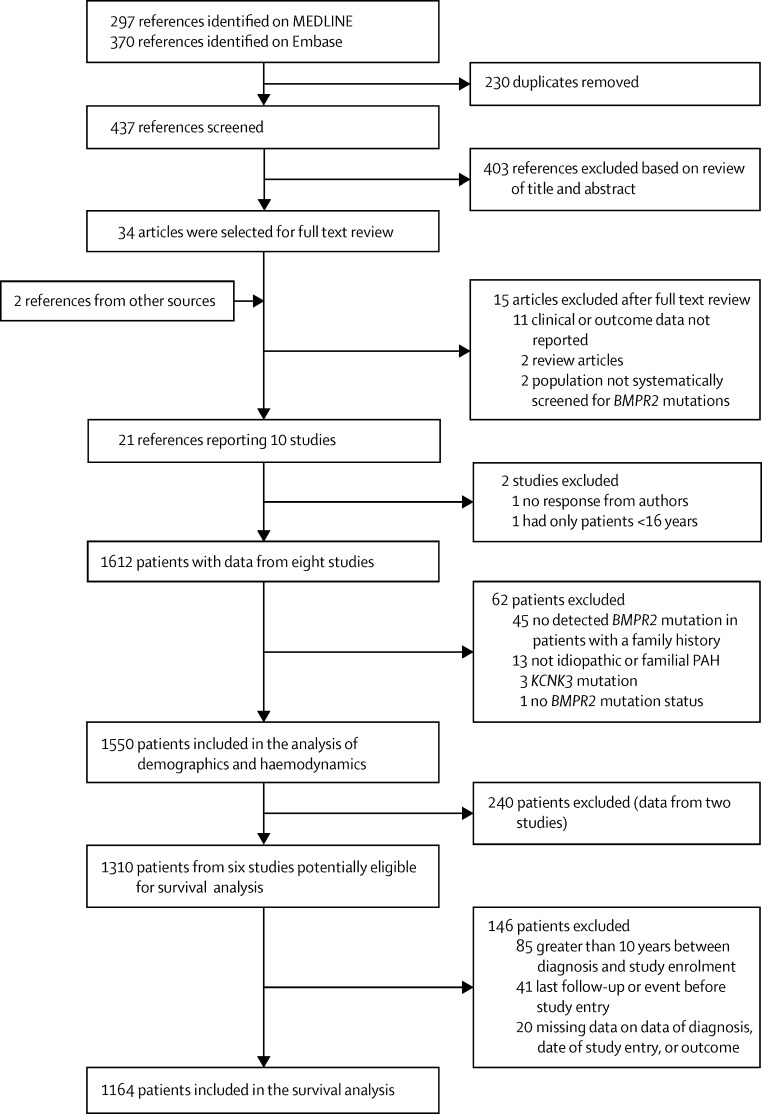
Methods: We analysed individual participant data of 1550 patients with idiopathic, heritable, and anorexigen-associated PAH from eight cohorts that had been systematically tested for BMPR2 mutations. The primary outcome was the composite of death or lung transplantation. All-cause mortality was the secondary outcome. Hazard ratios (HRs) for death or transplantation and all-cause mortality associated with the presence of BMPR2 mutation were calculated using Cox proportional hazards models stratified by cohort.
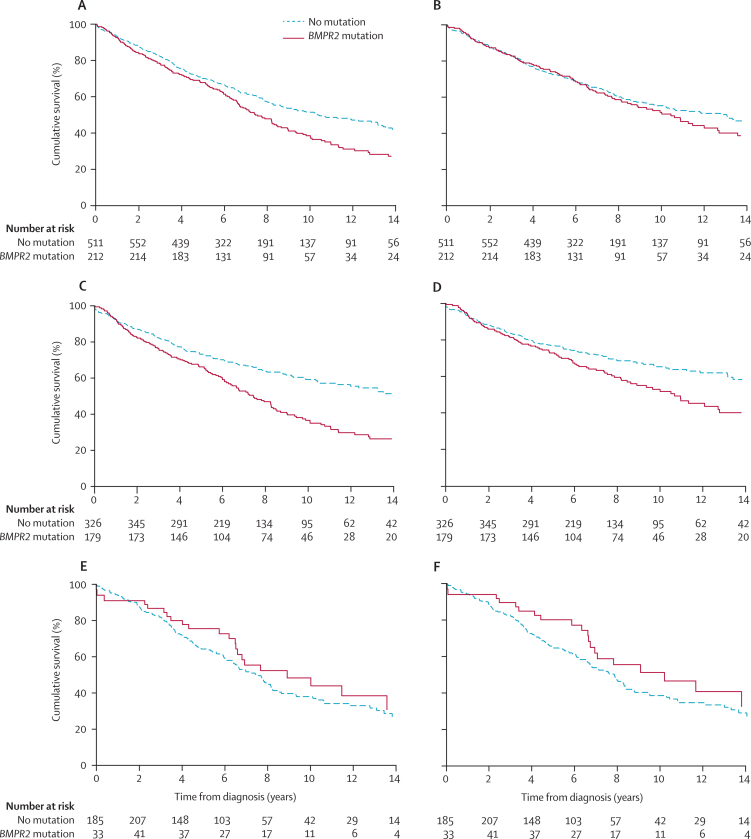
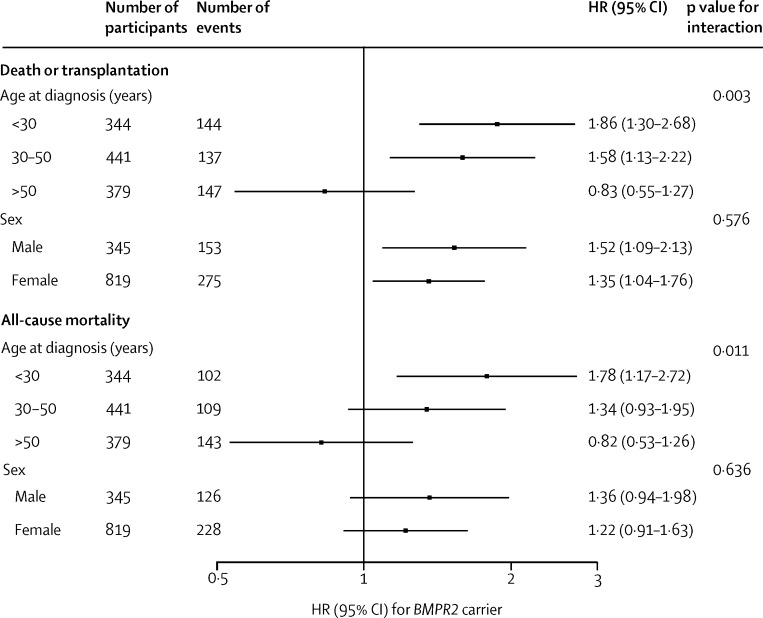
Findings: Overall, 448 (29%) of 1550 patients had a BMPR2 mutation. Mutation carriers were younger at diagnosis (mean age 35·4 [SD 14·8] vs 42·0 [17·8] years), had a higher mean pulmonary artery pressure (60·5 [13·8] vs 56·4 [15·3] mm Hg) and pulmonary vascular resistance (16·6 [8·3] vs 12·9 [8·3] Wood units), and lower cardiac index (2·11 [0·69] vs 2·51 [0·92] L/min per m(2); all p<0·0001). Patients with BMPR2 mutations were less likely to respond to acute vasodilator testing (3% [10 of 380] vs 16% [147 of 907]; p<0·0001). Among the 1164 individuals with available survival data, age-adjusted and sex-adjusted HRs comparing BMPR2 mutation carriers with non-carriers were 1·42 (95% CI 1·15-1·75; p=0·0011) for the composite of death or lung transplantation and 1·27 (1·00-1·60; p=0·046) for all-cause mortality. These HRs were attenuated after adjustment for potential mediators including pulmonary vascular resistance, cardiac index, and vasoreactivity. HRs for death or transplantation and all-cause mortality associated with BMPR2 mutation were similar in men and women, but higher in patients with a younger age at diagnosis (p=0·0030 for death or transplantation, p=0·011 for all-cause mortality).
Interpretation: Patients with PAH and BMPR2 mutations present at a younger age with more severe disease, and are at increased risk of death, and death or transplantation, compared with those without BMPR2 mutations.
Funding: Cambridge NIHR Biomedical Research Centre, Medical Research Council, British Heart Foundation, Assistance Publique-Hôpitaux de Paris, INSERM, Université Paris-Sud, Intermountain Research and Medical Foundation, Vanderbilt University, National Center for Advancing Translational Sciences, National Institutes of Health, National Natural Science Foundation of China, and Beijing Natural Science Foundation.
Copyright © 2016 Evans et al. Open Access article distributed under the terms of CC-BY. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
BMPR2 revisited: are bigger data better?Lancet Respir Med. 2016 Feb;4(2):87-9. doi: 10.1016/S2213-2600(16)00012-6. Epub 2016 Jan 19. Lancet Respir Med. 2016. PMID: 26795433 No abstract available.
References
-
- McLaughlin VV, McGoon MD. Pulmonary arterial hypertension. Circulation. 2006;114:1417–1431. - PubMed
-
- Humbert M, Morrell NW, Archer SL. Cellular and molecular pathobiology of pulmonary arterial hypertension. J Am Coll Cardiol. 2004;43:S13–S24. - PubMed
-
- Badesch DB, Champion HC, Sanchez MA. Diagnosis and assessment of pulmonary arterial hypertension. J Am Coll Cardiol. 2009;54:S55–S66. - PubMed
-
- Simonneau G, Gatzoulis MA, Adatia I. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2013;62:S34–S41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- RG/08/014/24067/BHF_/British Heart Foundation/United Kingdom
- G0800784/MRC_/Medical Research Council/United Kingdom
- MR/K020919/1/MRC_/Medical Research Council/United Kingdom
- RG/13/4/30107/BHF_/British Heart Foundation/United Kingdom
- MR/L003120/1/MRC_/Medical Research Council/United Kingdom
- CH/09/001/25945/BHF_/British Heart Foundation/United Kingdom
- R01 HL060056/HL/NHLBI NIH HHS/United States
- K23 HL098743/HL/NHLBI NIH HHS/United States
- SP/12/12/29836/BHF_/British Heart Foundation/United Kingdom
- UL1 TR000445/TR/NCATS NIH HHS/United States
- P01 HL108800/HL/NHLBI NIH HHS/United States
- G1000847/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
