

Racial and Ethnic Disparities in Mode of Anesthesia for Cesarean Delivery
- PMID: 26797554
- PMCID: PMC4724639
- DOI: 10.1213/ANE.0000000000000679
Racial and Ethnic Disparities in Mode of Anesthesia for Cesarean Delivery
Abstract
Background: Racial and ethnic disparities have been identified in the provision of neuraxial labor analgesia. These disparities may exist in other key aspects of obstetric anesthesia care. We sought to determine whether racial/ethnic disparities exist in mode of anesthesia for cesarean delivery (CD).
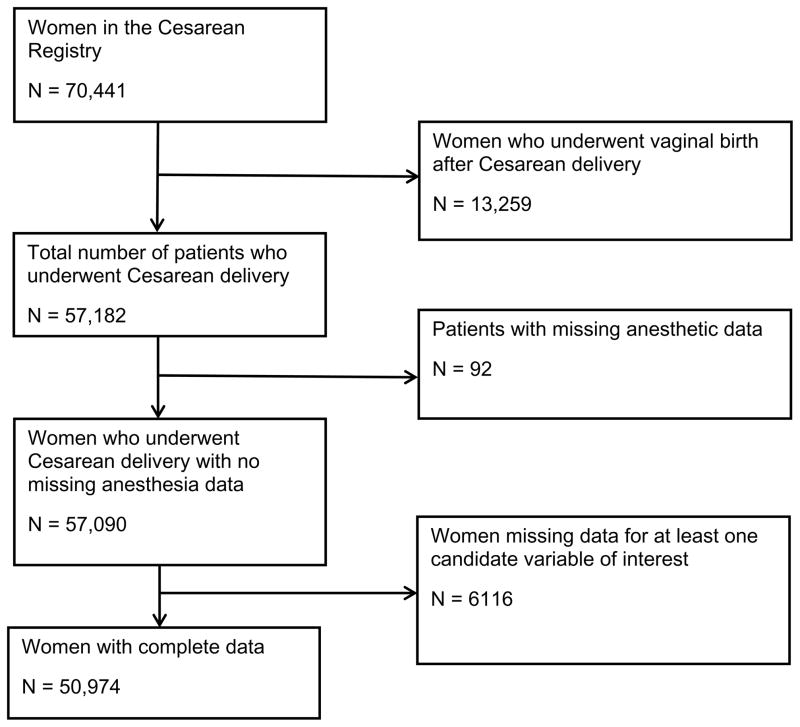
Methods: Women who underwent CD between 1999 and 2002 at 19 different obstetric centers in the United States were identified from the Maternal-Fetal Medicine Units Network Cesarean Registry. Race/ethnicity was categorized as: Caucasian, African American, Hispanic, and Non-Hispanic Others (NHOs). Mode of anesthesia was classified as neuraxial anesthesia (spinal, epidural, or combined spinal-epidural anesthesia) or general anesthesia. To account for obstetric and non-obstetric covariates that may have influenced mode of anesthesia, multiple logistic regression analyses were performed by using sequential sets of covariates.
Results: The study cohort comprised 50,974 women who underwent CD. Rates of general anesthesia among racial/ethnic groups were as follows: 5.2% for Caucasians, 11.3% for African Americans, 5.8% for Hispanics, and 6.6% for NHOs. After adjustment for obstetric and non-obstetric covariates, African Americans had the highest odds of receiving general anesthesia compared with Caucasians (adjusted odds ratio [aOR] = 1.7; 95% confidence interval [CI], 1.5-1.8; P < 0.001). The odds of receiving general anesthesia were also higher among Hispanics (aOR = 1.1; 95% CI, 1.0-1.3; P = 0.02) and NHOs (aOR = 1.2; 95% CI, 1.0-1.4; P = 0.03) compared with Caucasians, respectively. In our sensitivity analysis, we reconstructed the models after excluding women who underwent neuraxial anesthesia before general anesthesia. The adjusted odds of receiving general anesthesia were similar to those in the main analysis: African Americans (aOR = 1.7; 95% CI, 1.5-1.9; P < 0.001); Hispanics (aOR = 1.2; 95% CI, 1.1-1.4; P = 0.006); and NHOs (aOR = 1.2; 95% CI, 1.0-1.5; P = 0.05).
Conclusions: Based on data from the Cesarean Registry, African American women had the highest odds of undergoing general anesthesia for CD compared with Caucasian women. It is uncertain whether this disparity exists in current obstetric practice.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Comment in
-
Racial and Ethnic Disparities in General Anesthesia for Cesarean: What Are the Implications?Anesth Analg. 2016 Feb;122(2):297-8. doi: 10.1213/ANE.0000000000001103. Anesth Analg. 2016. PMID: 26797543 No abstract available.
References
-
- Practice guidelines for obstetric anesthesia: an updated report by the American Society of Anesthesiologists Task Force on Obstetric Anesthesia. Anesthesiology. 2007;106:843–63. - PubMed
-
- Jenkins JG, Khan MM. Anaesthesia for Caesarean section: a survey in a UK region from 1992 to 2002. Anaesthesia. 2003;58:1114–8. - PubMed
-
- Bucklin BA, Hawkins JL, Anderson JR, Ullrich FA. Obstetric anesthesia workforce survey: twenty-year update. Anesthesiology. 2005;103:645–53. - PubMed
-
- Hawkins JL, Chang J, Palmer SK, Gibbs CP, Callaghan WM. Anesthesia-related maternal mortality in the United States: 1979–2002. Obstet Gynecol. 2011;117:69–74. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
