

Efficacy and safety of betahistine treatment in patients with Meniere's disease: primary results of a long term, multicentre, double blind, randomised, placebo controlled, dose defining trial (BEMED trial)
- PMID: 26797774
- PMCID: PMC4721211
- DOI: 10.1136/bmj.h6816
Efficacy and safety of betahistine treatment in patients with Meniere's disease: primary results of a long term, multicentre, double blind, randomised, placebo controlled, dose defining trial (BEMED trial)
Abstract
Study question: What is the long term efficacy of betahistine dihydrochloride on the incidence of vertigo attacks in patients with Meniere's disease, compared with placebo?
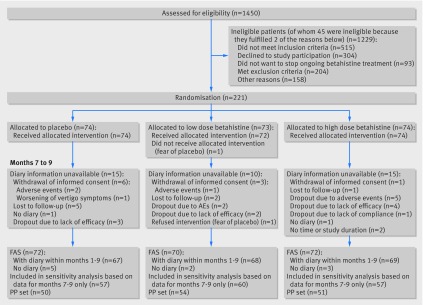
Methods: The BEMED trial is a multicentre, double blind, randomised, placebo controlled, three arm, parallel group, phase III, dose defining superiority trial conducted in 14 German tertiary referral centres (for neurology or ear, nose, and throat). Adults aged 21-80 years (mean age 56 years) with definite unilateral or bilateral Meniere's disease were recruited from March 2008 to November 2012. Participants received placebo (n=74), low dose betahistine (2 × 24 mg daily, (n=73)), or high dose betahistine (3 × 48 mg daily, (n=74)) over nine months. The primary outcome was the number of attacks per 30 days, based on patients' diaries during a three month assessment period at months seven to nine. An internet based randomisation schedule performed a concealed 1:1:1 allocation, stratified by study site. Secondary outcomes included the duration and severity of attacks, change in quality of life scores, and several observer-reported parameters to assess changes in audiological and vestibular function.
Study answer and limitations: Incidence of attacks related to Meniere's disease did not differ between the three treatment groups (P=0.759). Compared with placebo, attack rate ratios were 1.036 (95% confidence interval 0.942 to 1.140) and 1.012 (0.919 to 1.114) for low dose and high dose betahistine, respectively. The overall monthly attack rate fell significantly by the factor 0.758 (0.705 to 0.816; P<0.001). The population based, mean monthly incidence averaged over the assessment period was 2.722 (1.304 to 6.309), 3.204 (1.345 to 7.929), and 3.258 (1.685 to 7.266) for the placebo, low dose betahistine, and high dose betahistine groups, respectively. Results were consistent for all secondary outcomes. Treatment was well tolerated with no unexpected safety findings. Without a control group of patients who did not receive any intervention to follow the natural course of the disease, the placebo effect could not be accurately assessed and differentiated from spontaneous remission and fluctuation of symptoms.
What this study adds: Current evidence is limited as to whether betahistine prevents vertigo attacks caused by Meniere's disease, compared with placebo. The trial provides information on symptom relief on placebo intervention which is relevant for the design of future studies on potential disease modifying treatments in patients with Meniere's disease.
Funding, competing interests, data sharing: Support from the German Federal Ministry of Education and Research (BMBF support code 01KG0708). Potential competing interests have been reported in full at the end of the paper on thebmj.com. Data are available from the corresponding author (Michael.Strupp@med.uni-muenchen.de) or biostatistician (mansmann@ibe.med.uni-muenchen.de). Study registration EudraCT no 2005-000752-32; ISRCTN no ISRCTN44359668.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures


Comment in
-
Therapeutic illusion: another frontier in Ménière's disease.Ann Transl Med. 2016 Oct;4(Suppl 1):S63. doi: 10.21037/atm.2016.10.61. Ann Transl Med. 2016. PMID: 27868031 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical