

Clinical features predict responsiveness to imatinib in platelet-derived growth factor receptor-alpha-negative hypereosinophilic syndrome
- PMID: 26797802
- PMCID: PMC6109366
- DOI: 10.1111/all.12843
Clinical features predict responsiveness to imatinib in platelet-derived growth factor receptor-alpha-negative hypereosinophilic syndrome
Abstract
Background: With the exception of the presence of the FIP1L1-PDGFRA fusion gene, little is known about predictors of imatinib response in clinically-defined hypereosinophilic syndrome (HES).
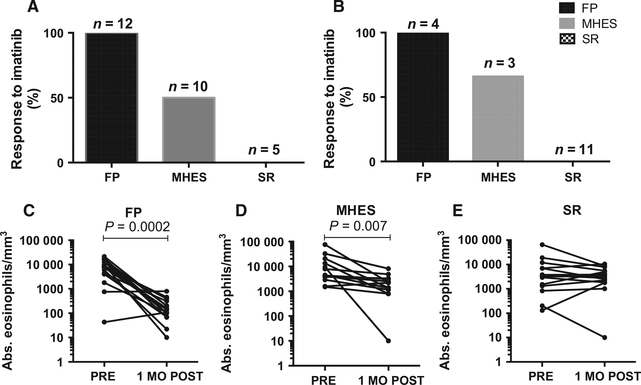
Methods: Subjects with FIP1L1-PDGFRA-myeloid neoplasm (FP; n =12), PDGFRA-negative HES with ≥4 criteria suggestive of a myeloid neoplasm (MHES; n =10), or steroid-refractory PDGFRA-negative HES with <4 myeloid criteria (SR; n = 5) were enrolled in a prospective study of imatinib therapy (NCT00044304: registered at clinicaltrials.gov). The primary outcome was an eosinophil count <1.5 × 109/L at one month and improvement of clinical symptoms. Clinical, molecular, and bone marrow responses to imatinib were assessed. A retrospective cohort of 18 subjects with clinically-defined HES who received imatinib (300-400 mg daily ≥ 1 month) were classified according to the criteria used in the prospective study.
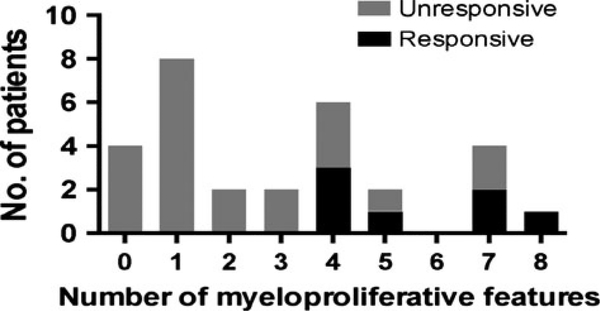
Results: Overall, imatinib response rates were 100% in the FP group (n = 16), 54% in the MHES group (n = 13) and 0% in the SR group (n = 16). The presence of ≥ 4 myeloid features was the sole predictor of response. After ≥ 18 months in complete remission, imatinib was tapered and discontinued in 8 FP and 1 MHES subjects. Seven subjects (6 FP, 1 MHES) remain in remission off therapy for a median of 29 months (range 14-36).
Conclusions: Clinical features of MHES predict imatinib response in PDGFRA-negative HES.
Trial registration: ClinicalTrials.gov NCT00044304 NCT00001406.
Keywords: PDGFRA-negative; eosinophilia; hypereosinophilic syndrome; imatinib; myeloid neoplasm.
Published 2016. This article is a U.S. Government work and is in the public domain in the USA.
Conflict of interest statement
Conflicts of interest
No conflicts of interest are reported for any of the authors.
Figures
References
-
- Baccarani M, Cilloni D, Rondoni M, Ottaviani E, Messa F, Merante S et al. The efficacy of imatinib mesylate in patients with FIP1L1-PDGFRalpha-positive hypere-osinophilic syndrome. Results of a multicenter prospective study. Haematologica 2007;92:1173–1179. - PubMed
-
- Cools J, DeAngelo DJ, Gotlib J, Stover EH, Legare RD, Cortes J et al. A tyrosine kinase created by fusion of the PDGFRA and FIP1L1 genes as a therapeutic target of imatinib in idiopathic hypereosinophilic syndrome. N Engl J Med 2003;348:1201–1214. - PubMed
-
- Helbig G, Hus M, Halasz M, Dudzinski M, Wieclawek A, Stachowicz M et al. Imatinib mesylate may induce long-term clinical response in FIP1L1-PDGFRalpha-negative hypereosinophilic syndrome. Med Oncol 2012;29:1073–1076. - PubMed
-
- Klion AD, Robyn J, Akin C, Noel P, Brown M, Law M et al. Molecular remission and reversal of myelofibrosis in response to imatinib mesylate treatment in patients with the myeloproliferative variant of hypere-osinophilic syndrome. Blood 2004; 103:473–478. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
