

Addition of a Medial Locking Plate to an In Situ Lateral Locking Plate Results in Healing of Distal Femoral Nonunions
- PMID: 26797911
- PMCID: PMC4868169
- DOI: 10.1007/s11999-016-4709-3
Addition of a Medial Locking Plate to an In Situ Lateral Locking Plate Results in Healing of Distal Femoral Nonunions
Abstract
Background: Nonunion of the distal femur after lateral plating is associated with axial malalignment, chronic pain, loss of ambulatory function, and decreased knee ROM. The addition of a medial locking plate with autogenous bone grafting can provide greater stability to allow bone healing and may be used to achieve union in these challenging cases.
Questions/purposes: We wished to determine (1) the proportion of patients who achieve radiographic signs of osseous union for distal femoral nonunions with an in situ lateral plate after treatment with addition of a medial locking plate and autogenous bone grafting, and (2) the frequency and types of complications associated with this treatment.
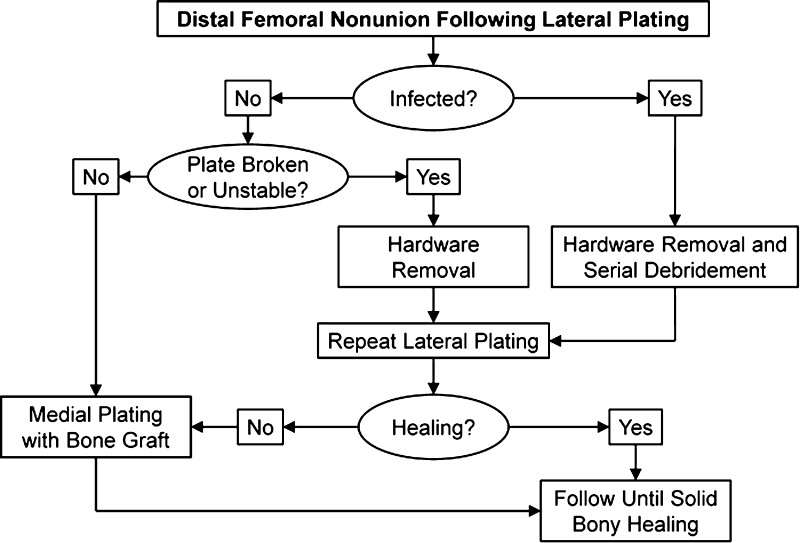
Methods: Between 2007 and 2013, we treated 22 patients for 23 distal femoral nonunions, defined as an unhealed fracture with no radiographic signs of osseous union at a mean of 16 months (SD, 13 months) after injury. During that time, we used a treatment algorithm consisting of treatment in one or two stages. The single-stage procedure performed in 16 aseptic nonunions with a stable lateral plate involved addition of a medial locking plate and autogenous bone graft. A two-stage treatment performed in seven nonunions with lateral plate failure involved placement of a new lateral locking plate followed by addition of a medial locking plate with autogenous bone graft at least 2 months after the first procedure. Of the 22 patients treated, 20 had a median followup of 18 months (SD, 6-94 months). We defined osseous union by bridging bone on three of four cortices with absence of a radiolucent line or more than 25% cross-sectional area of bridging bone via CT.
Results: Twenty of the 21 nonunions attained radiographic signs of osseous union by 12 months. Six of the 20 patients experienced complications: one patient had a persistent nonunion; four patients underwent removal of symptomatic hardware; and one patient experienced skin breakdown at the bone graft harvest site.
Conclusions: A very high proportion of patients achieve union when using medial locking plates to treat distal femoral nonunions after lateral plating of the original injury. Addition of bone graft, staged reconstruction, and revision of the initial lateral plate is indicated when the nonunion is associated with fatigue failure of the initial lateral plate.
Level of evidence: Level IV, therapeutic study.
Figures

Comment in
-
CORR Insights(®): Addition of a Medial Locking Plate to an In Situ Lateral Locking Plate Results in Healing of Distal Femoral Nonunions.Clin Orthop Relat Res. 2016 Jun;474(6):1506-7. doi: 10.1007/s11999-016-4745-z. Epub 2016 Mar 28. Clin Orthop Relat Res. 2016. PMID: 27020424 Free PMC article. No abstract available.
Similar articles
-
What Is the Likelihood of Union and Frequency of Complications After Parallel Plating and Supplemental Bone Grafting for Resistant Distal Femoral Nonunions?Clin Orthop Relat Res. 2024 Feb 1;482(2):362-372. doi: 10.1097/CORR.0000000000002809. Epub 2023 Aug 28. Clin Orthop Relat Res. 2024. PMID: 37638842 Free PMC article.
-
Treatment of Distal Femur Nonunion Following Initial Fixation with a Lateral Locking Plate.Orthop Surg. 2016 Aug;8(3):323-30. doi: 10.1111/os.12257. Orthop Surg. 2016. PMID: 27627715 Free PMC article.
-
Treatment of distal femoral nonunion with internal fixation, cortical allograft struts, and autogenous bone-grafting.J Bone Joint Surg Am. 2003 Mar;85(3):436-40. doi: 10.2106/00004623-200303000-00006. J Bone Joint Surg Am. 2003. PMID: 12637428
-
Endosteal plating for the treatment of malunions and nonunions of distal femur fractures.Eur J Orthop Surg Traumatol. 2023 Aug;33(6):2243-2251. doi: 10.1007/s00590-022-03458-x. Epub 2022 Dec 21. Eur J Orthop Surg Traumatol. 2023. PMID: 36539626 Review.
-
Diagnostic and treatment modalities in nonunions of the femoral shaft: a review.Injury. 2012 Jul;43(7):980-8. doi: 10.1016/j.injury.2011.06.030. Epub 2011 Jul 8. Injury. 2012. PMID: 21741650 Review.
Cited by
-
Augmented fixation in distal femur fractures: how does it fare?Singapore Med J. 2023 Oct;64(10):634-639. doi: 10.11622/smedj.2022086. Singapore Med J. 2023. PMID: 35739631 Free PMC article. No abstract available.
-
Smoking and obesity influence the risk of nonunion in lateral opening wedge, closing wedge and torsional distal femoral osteotomies.Knee Surg Sports Traumatol Arthrosc. 2018 Sep;26(9):2551-2557. doi: 10.1007/s00167-017-4754-9. Epub 2017 Nov 8. Knee Surg Sports Traumatol Arthrosc. 2018. PMID: 29119287
-
Management of Distal Femoral Non-union: A Systematic Review.Indian J Orthop. 2024 Jun 22;58(12):1686-1723. doi: 10.1007/s43465-024-01205-4. eCollection 2024 Dec. Indian J Orthop. 2024. PMID: 39664354 Free PMC article. Review.
-
The impact of medial-first dual plating for reduction of distal femoral fractures: a retrospective comparative cohort study.Sci Rep. 2025 May 2;15(1):15454. doi: 10.1038/s41598-025-99271-7. Sci Rep. 2025. PMID: 40316699 Free PMC article.
-
The Influence of Fracture Defect Size on Treatment Outcomes in Distal Femur Fractures: A Comparative Study Between Lateral Locking Plate and Double Plate Fixation.Orthop Surg. 2025 Aug;17(8):2435-2444. doi: 10.1111/os.70103. Epub 2025 Jun 26. Orthop Surg. 2025. PMID: 40574252 Free PMC article.
References
-
- Brinker MR, O’Connor DP. Nonunions: Evaluation and Treatment. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, Krettek C, editors. Skeletal Trauma: Basic Science, Management, and Reconstruction. 4. Philadelphia, PA: W.B. Saunders; 2009. pp. 615–707.
-
- Cavusoglu AT, Ozsoy MH, Dincel VE, Sakaogullari A, Basarir K, Ugurlu M. The use of a low-profile Ilizarov external fixator in the treatment of complex fractures and non-unions of the distal femur. Acta Orthop Belg. 2009;75:209–218. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
