

Early hepatocellular carcinoma with high-grade atypia in small vaguely nodular lesions
- PMID: 26797961
- PMCID: PMC4832853
- DOI: 10.1111/cas.12893
Early hepatocellular carcinoma with high-grade atypia in small vaguely nodular lesions
Abstract
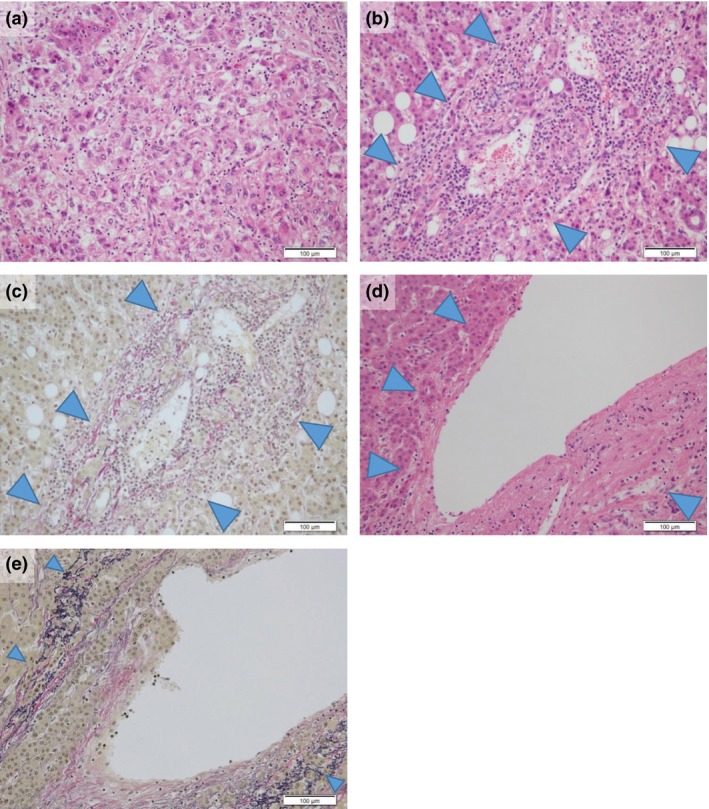
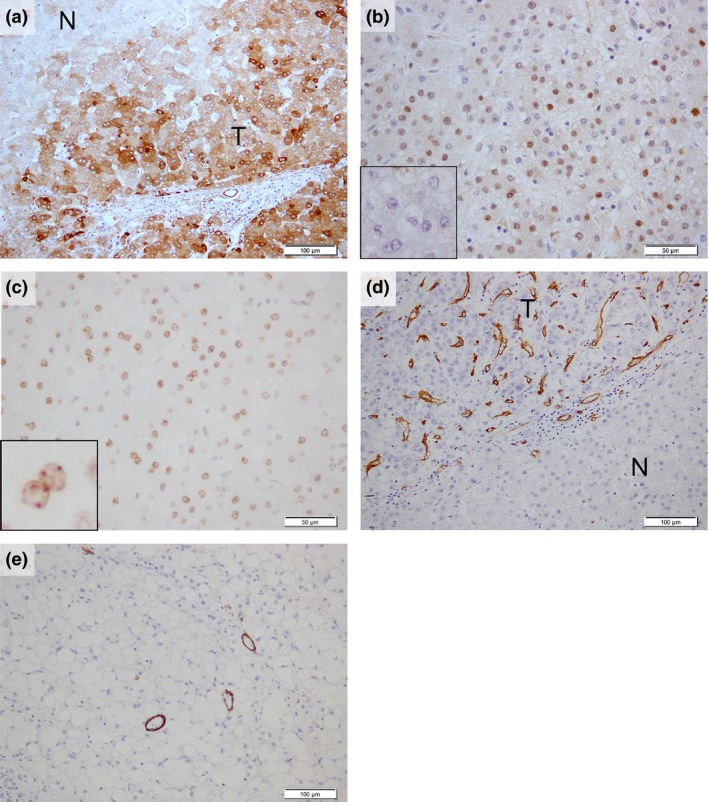
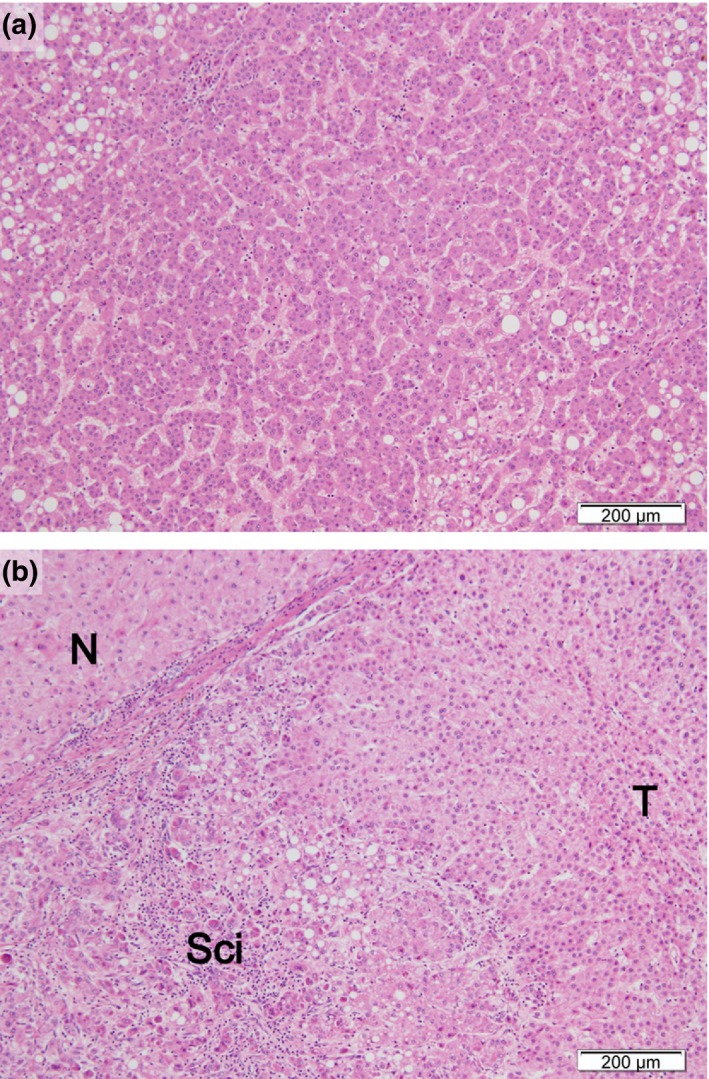
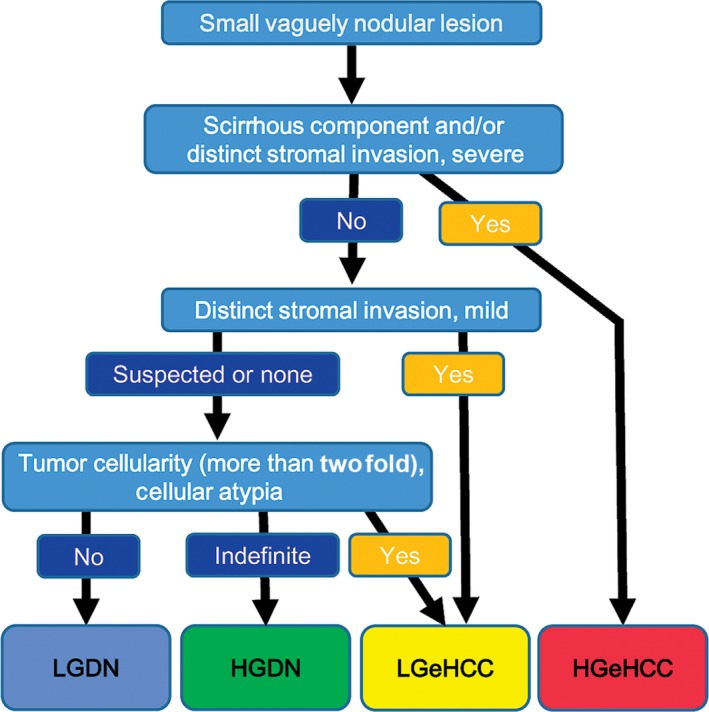
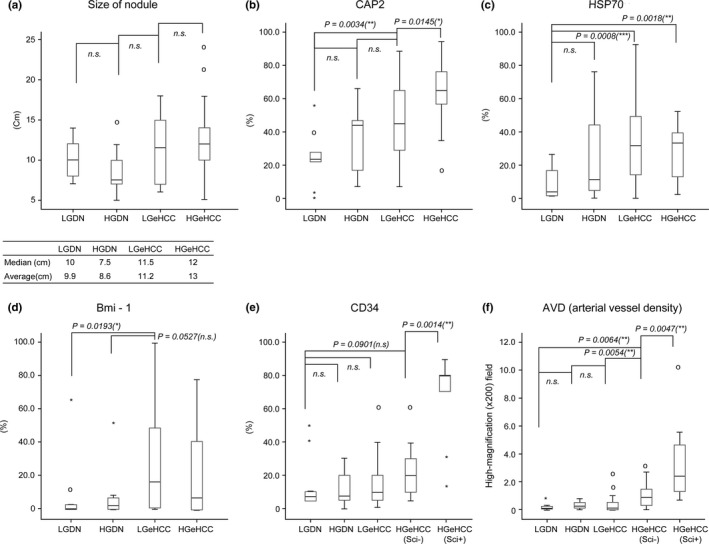
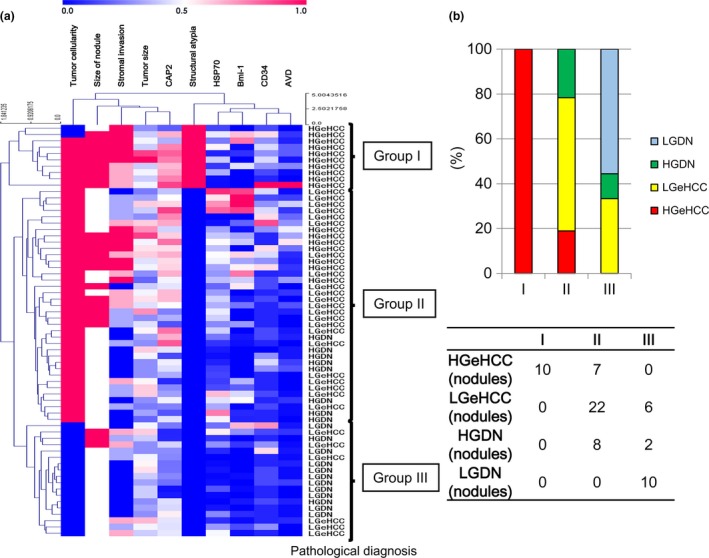
Multistep hepatocarcinogenesis progresses from dysplastic nodules to early hepatocellular carcinoma (eHCC) and to advanced HCC. The aim of the present study was to investigate the detailed histopathological features of eHCC. We investigated 66 small vaguely nodular lesions resected from 40 patients. The degree of cellular and structural atypia and stromal invasion were assessed. The immunohistochemical expression of HCC-related markers adenylate cyclase-associated protein 2 (CAP2), heat shock protein 70 (HSP70), Bmi-1, CD34 and h-caldesmon were evaluated. Of the 66 nodules, 10 were diagnosed as low-grade dysplastic nodules (LGDN), 10 as high-grade dysplastic nodules (HGDN) and 46 as eHCC. Among the 46 eHCC, 18 nodules (39.1%) showed marked stromal invasion and/or the presence of the scirrhous component and were subclassified as high-grade eHCC (HGeHCC). The remaining 28 eHCC, which lacked these features, were subclassified as low-grade eHCC (LGeHCC) and were examined further. HGeHCC showed high levels of cellular and structural atypia and large tumor size. The immunohistochemical expression of CAP2 and the area of sinusoidal vascularization showed increases from LGDN to HGeHCC. The density of arterial tumor vessels was high in HGeHCC compared with other nodule types. Cluster analysis of these parameters subclassified 65 nodules into HGeHCC-dominant, LGeHCC and HGDN-dominant, and LGDN-dominant groups. These results indicate the increased malignant potential of HGeHCC and suggest that it is already a transitional stage to advanced HCC. We consider that our grading classification system may be valuable for considering treatment strategies for eHCC around 2 cm in diameter.
Keywords: Cyclase-associated protein 2; early hepatocellular carcinoma; high grade; scirrhous component; stromal invasion.
© 2016 The Authors. Cancer Science published by John Wiley & Sons Australia, Ltd on behalf of Japanese Cancer Association.
Figures
Similar articles
-
Morphophenotypic changes in human multistep hepatocarcinogenesis with translational implications.J Hepatol. 2016 Jan;64(1):87-93. doi: 10.1016/j.jhep.2015.08.031. Epub 2015 Sep 5. J Hepatol. 2016. PMID: 26343958
-
Specific patterns of PIWI-interacting small noncoding RNA expression in dysplastic liver nodules and hepatocellular carcinoma.Oncotarget. 2016 Aug 23;7(34):54650-54661. doi: 10.18632/oncotarget.10567. Oncotarget. 2016. PMID: 27429044 Free PMC article.
-
Early stages of multistep hepatocarcinogenesis: adenomatous hyperplasia and early hepatocellular carcinoma.Hum Pathol. 1991 Feb;22(2):172-8. doi: 10.1016/0046-8177(91)90039-r. Hum Pathol. 1991. PMID: 1848205
-
Update on precursor and early lesions of hepatocellular carcinomas.Arch Pathol Lab Med. 2011 Jun;135(6):704-15. doi: 10.5858/2010-0524-RA.1. Arch Pathol Lab Med. 2011. PMID: 21631263 Review.
-
Atypical large well-differentiated hepatocellular carcinoma with benign nature: a new clinical entity.Intervirology. 2004;47(3-5):227-37. doi: 10.1159/000078475. Intervirology. 2004. PMID: 15383732 Review.
Cited by
-
The clinicopathological characterization of small hepatocellular carcinoma with fibrous stroma.Int J Clin Exp Pathol. 2018 Oct 1;11(10):4806-4816. eCollection 2018. Int J Clin Exp Pathol. 2018. PMID: 31949555 Free PMC article.
-
Expression of hnRNPK & Claudin-4 in HCV-Induced Early HCC and Adjacent Liver Tissue.Open Access Maced J Med Sci. 2017 Jul 31;5(5):595-602. doi: 10.3889/oamjms.2017.092. eCollection 2017 Aug 15. Open Access Maced J Med Sci. 2017. PMID: 28932298 Free PMC article.
-
Endoplasmic Reticulum Stress Induces CAP2 Expression Promoting Epithelial-Mesenchymal Transition in Liver Cancer Cells.Mol Cells. 2021 Aug 31;44(8):569-579. doi: 10.14348/molcells.2021.0031. Mol Cells. 2021. PMID: 34294609 Free PMC article.
-
Current status and new directions for hepatocellular carcinoma diagnosis.Liver Res. 2024 Dec 5;8(4):218-236. doi: 10.1016/j.livres.2024.12.001. eCollection 2024 Dec. Liver Res. 2024. PMID: 39958920 Free PMC article. Review.
-
Current Concepts of Precancerous Lesions of Hepatocellular Carcinoma: Recent Progress in Diagnosis.Diagnostics (Basel). 2023 Mar 23;13(7):1211. doi: 10.3390/diagnostics13071211. Diagnostics (Basel). 2023. PMID: 37046429 Free PMC article. Review.
References
-
- Takayama T, Makuuchi M, Hirohashi S et al Malignant transformation of adenomatous hyperplasia to hepatocellular carcinoma. Lancet 1990; 336: 1150–3. - PubMed
-
- Sakamoto M, Hirohashi S, Shimosato Y. Early stages of multistep hepatocarcinogenesis: adenomatous hyperplasia and early hepatocellular carcinoma. Hum Pathol 1991; 22: 172–8. - PubMed
-
- Sakamoto M. Pathology of early hepatocellular carcinoma. Hepatol Res 2007; 37(Suppl 2): S135–8. - PubMed
-
- Sakamoto M, Effendi K, Masugi Y. Molecular diagnosis of multistage hepatocarcinogenesis. Jpn J Clin Oncol 2010; 40: 891–6. - PubMed
-
- International Consensus Group for Hepatocellular Neoplasia . Pathologic diagnosis of early hepatocellular carcinoma: a report of the international consensus group for hepatocellular neoplasia. Hepatology 2009; 49: 658–64. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
