

The Time Is Right for a New Classification System for Diabetes: Rationale and Implications of the β-Cell-Centric Classification Schema
- PMID: 26798148
- PMCID: PMC5317235
- DOI: 10.2337/dc15-1585
The Time Is Right for a New Classification System for Diabetes: Rationale and Implications of the β-Cell-Centric Classification Schema
Abstract
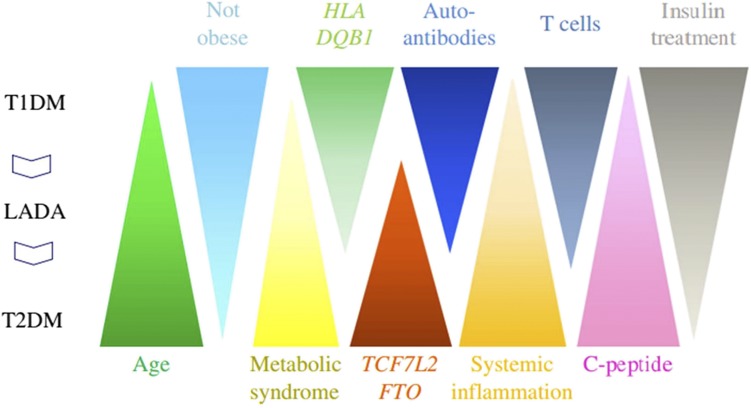
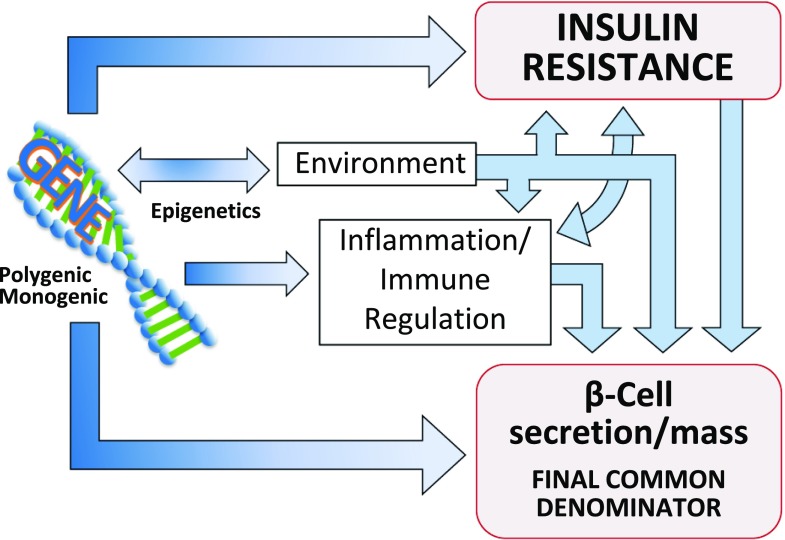
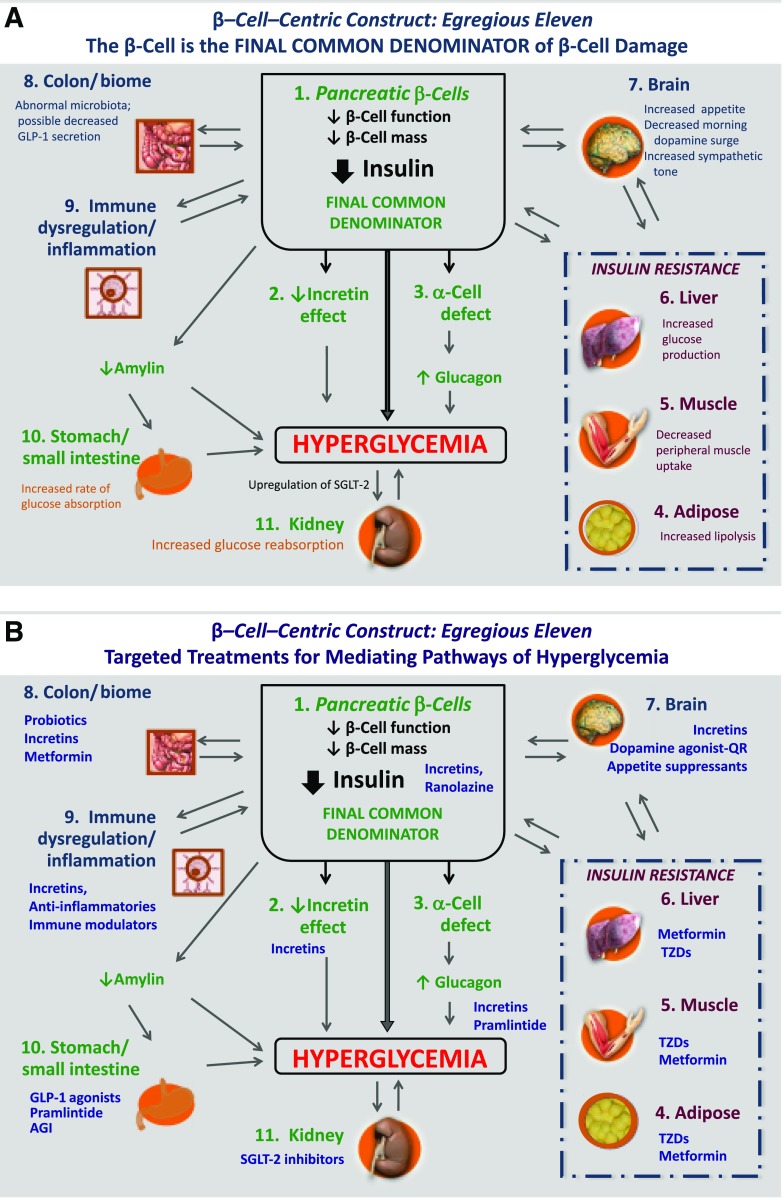
The current classification system presents challenges to the diagnosis and treatment of patients with diabetes mellitus (DM), in part due to its conflicting and confounding definitions of type 1 DM, type 2 DM, and latent autoimmune diabetes of adults (LADA). The current schema also lacks a foundation that readily incorporates advances in our understanding of the disease and its treatment. For appropriate and coherent therapy, we propose an alternate classification system. The β-cell-centric classification of DM is a new approach that obviates the inherent and unintended confusions of the current system. The β-cell-centric model presupposes that all DM originates from a final common denominator-the abnormal pancreatic β-cell. It recognizes that interactions between genetically predisposed β-cells with a number of factors, including insulin resistance (IR), susceptibility to environmental influences, and immune dysregulation/inflammation, lead to the range of hyperglycemic phenotypes within the spectrum of DM. Individually or in concert, and often self-perpetuating, these factors contribute to β-cell stress, dysfunction, or loss through at least 11 distinct pathways. Available, yet underutilized, treatments provide rational choices for personalized therapies that target the individual mediating pathways of hyperglycemia at work in any given patient, without the risk of drug-related hypoglycemia or weight gain or imposing further burden on the β-cells. This article issues an urgent call for the review of the current DM classification system toward the consensus on a new, more useful system.
© 2016 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered.
Figures
Comment in
-
Comment on Schwartz et al. The Time Is Right for a New Classification System for Diabetes: Rationale and Implications of the β-Cell-Centric Classification Schema. Diabetes Care 2016;39:179-186.Diabetes Care. 2016 Aug;39(8):e128. doi: 10.2337/dc16-0162. Diabetes Care. 2016. PMID: 27457643 No abstract available.
-
Response to Comment on Schwartz et al. The Time Is Right for a New Classification System for Diabetes: Rationale and Implications of the β-Cell-Centric Classification Schema. Diabetes Care 2016;39:179-186.Diabetes Care. 2016 Aug;39(8):e129-30. doi: 10.2337/dci16-0011. Diabetes Care. 2016. PMID: 27457644 No abstract available.
References
-
- Leslie RD, Palmer J, Schloot NC, Lernmark A. Diabetes at the crossroads: relevance of disease classification to pathophysiology and treatment. Diabetologia. 24 October 2015. [Epub ahead of print] - PubMed
-
- Grant SFA, Hakonarson H, Schwartz S. Can the genetics of type 1 and type 2 diabetes shed light on the genetics of latent autoimmune diabetes in adults? Endocr Rev 2010;31:183–193 - PubMed
-
- Rolandsson O, Palmer JP. Latent autoimmune diabetes in adults (LADA) is dead: long live autoimmune diabetes! Diabetologia 2010;53:1250–1253 - PubMed
-
- Basile KJ, Guy VC, Schwartz S, Grant SFA. Overlap of genetic susceptibility to type 1 diabetes, type 2 diabetes, and latent autoimmune diabetes in adults. Curr Diab Rep 2014;14:550. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
