

Review
doi: 10.12945/j.aorta.2013.13-052.
eCollection 2013 Oct.
Lessons from Animal Models of Arterial Aneurysm
Affiliations
- PMID: 26798701
- PMCID: PMC4682768
- DOI: 10.12945/j.aorta.2013.13-052
Item in Clipboard
Review
Lessons from Animal Models of Arterial Aneurysm
Aorta (Stamford).
.
Abstract
We review the results from the most common animal models of arterial aneurysm, including recent findings from our novel, laparoscopy-based pig model of abdominal aortic aneurysm, that contribute important insights into early pathogenesis. We emphasize the relevance of these findings for evaluation of treatment protocols and novel device prototypes for mechanism-based prevention of progression and rupture.
Keywords: Abdominal aortic aneurysm; Animal models; Arterial aneurysm; Periarterial calcium chloride.
Figures
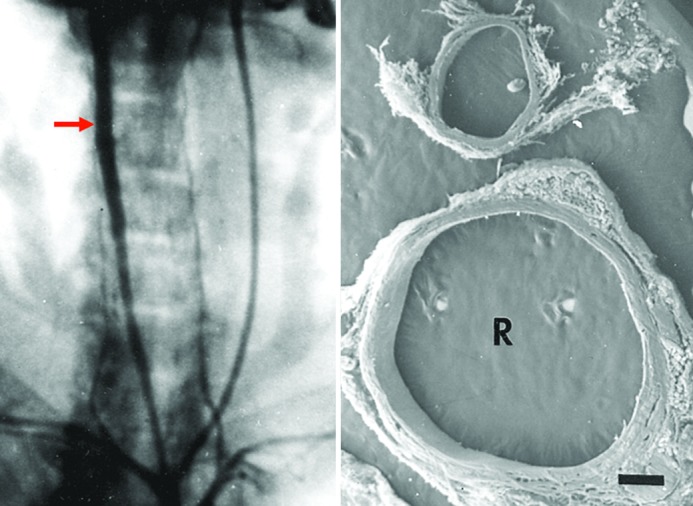
Periarterial calcium chloride. Left, Anteroposterior angiographic projection 3 weeks after a single, periarterial application of CaCl2 to the right common carotid artery of a rabbit. Note aneurysmal dilatation (arrow). Right, Scanning electron micrograph of cross-sections of the common carotid arteries of a rabbit 6 weeks after periarterial application of calcium chloride to the right vessel (R). Note marked dilatation compared with the contralateral, control vessel to which NaCl was applied (profile above) (15×). Reprinted with permission from Gertz et al., J Clin Invest. 1988;81:649-656.
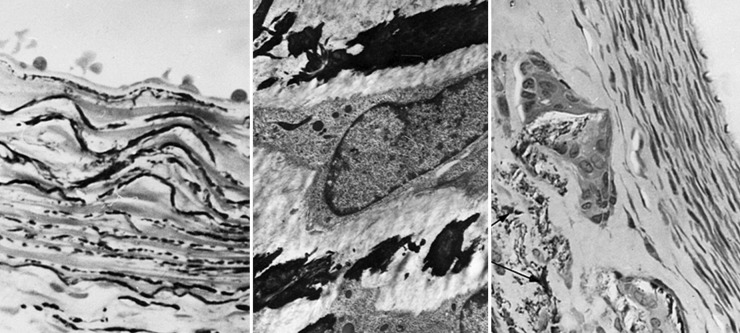
Periarterial calcium chloride. Left, Light microscopic section through the rabbit right common carotid artery (RCCA) 3 days after periarterial CaCl2 showing calcium precipitation within the internal elastic lamina and elastic layers of the media (Von Kossa, 640×). Middle, Transmission electron micrograph (pyroantimonate stain) of a CCA 1 week after CaCl2 showing calcium deposits (black) within the medial elastica (4200×). Right, RCCA 6 weeks after CaCl2 application showing calcium precipitation within the media with giant cells showing central vacuolization and engulfment of fragmented calcium-elastica beneath an area of intimal proliferation (Von Kossa, 350×). Reprinted with permission from Gertz et al., J Clin Invest. 1988;81:649-656.
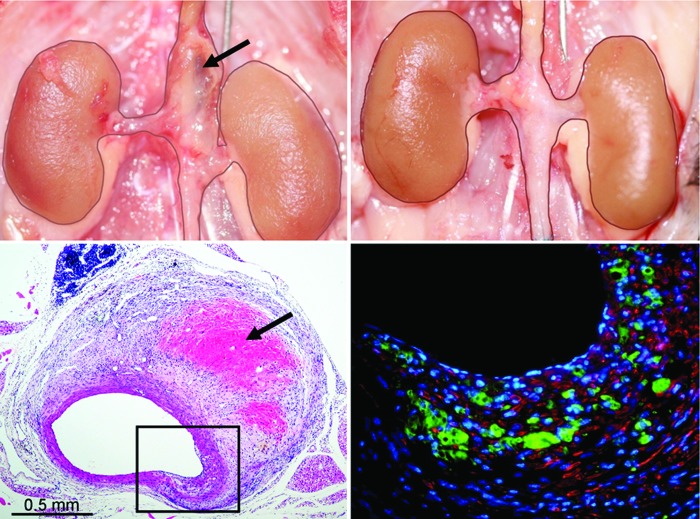
Suprarenal AAA 4 weeks after angiotensin-II (Ang-II) infusion in the apo-e−/− mouse (top left) not present in a similar mouse treated with low-level laser irradiation (LLLI) (top right). Needle standard is 0.5 mm. Note hemorrhage into the wall in the macroscopic (upper left, arrow) and H&E section (lower left; arrow) of the suprarenal segment of a nontreated Ang-II-infused mouse. The immunofluorescent stained section (lower right) of the boxed-in area of transmural disruption shows marked infiltration of MAC-2+ macrophages (green) in the area of the fragmented media (red = α-actin positive smooth muscle cells). Reprinted with permission from Gavish et al., Lasers in Surgery and Medicine. 2012;44:664–674.
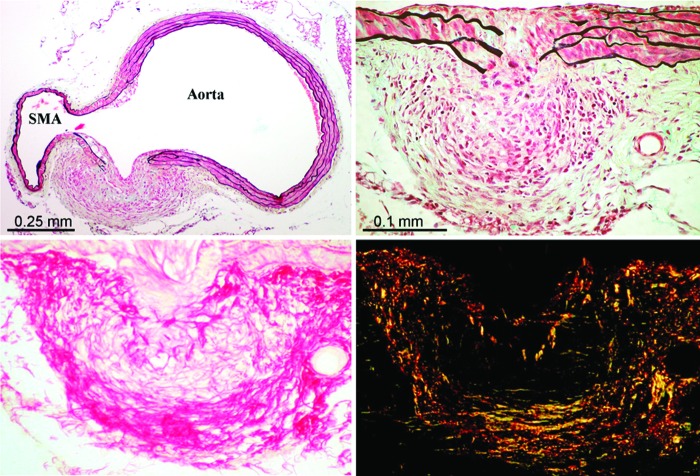
Suprarenal abdominal aorta of LLL-treated Ang-II-infused apo-e−/− mouse showing marked transmural disruption in the vicinity of the orifice of the superior mesenteric artery (SMA) with reactive fibromuscular hyperplasia appearing to wall off the medial defect preventing significant aneurysmal dilatation (top left and right; Movat pentachrome stain). Top right is a section immediately adjacent to that shown in the top left. Note the marked infiltration of inflammatory cells in the area of the disrupted media with macrophages and giant cells (arrow) at the site of fragmented elastic lamellae and injured smooth muscle cells. Lower panel shows the extensive collagen matrix formation in this reactive, “walling off” area (lower left = picrosirius red [PSR] stain for collagen in nonpolarized light; lower right = PSR stain viewed with polarized light). Reprinted with permission from Gavish et al., Lasers in Surgery and Medicine 2012;44:664–674.
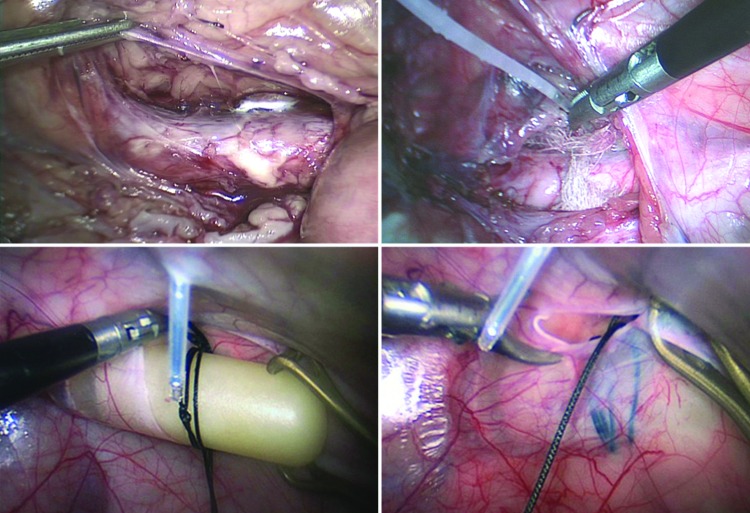
Images of the porcine model of experimental AAA showing laparoscopic exposure of the infrarenal abdominal aorta (top left), periarterial insertion of gauze and application of CaCl2 (top right), retroperitoneal insertion of angiotensin-II-filled osmotic minipump (bottom left), and closure of the peritoneum with the pump seen behind (bottom right).
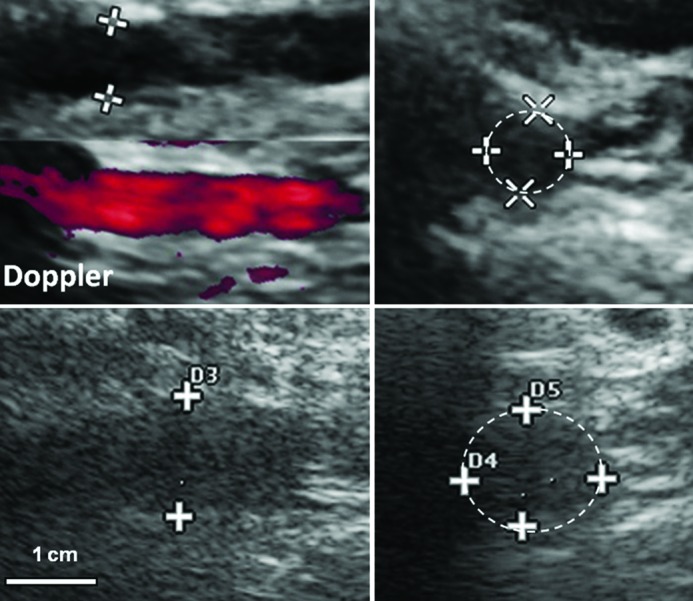
B-mode ultrasound before (top) and 4 weeks after (bottom) laparoscopic induction of AA(A). Left, Longitudinal views. Right, Cross-sections of infrarenal aorta at site of maximum cross-sectional diameter. This pig died from ruptured AAA at 5 weeks. A 5-9 MHz linear-array ultrasonographic probe is shown.
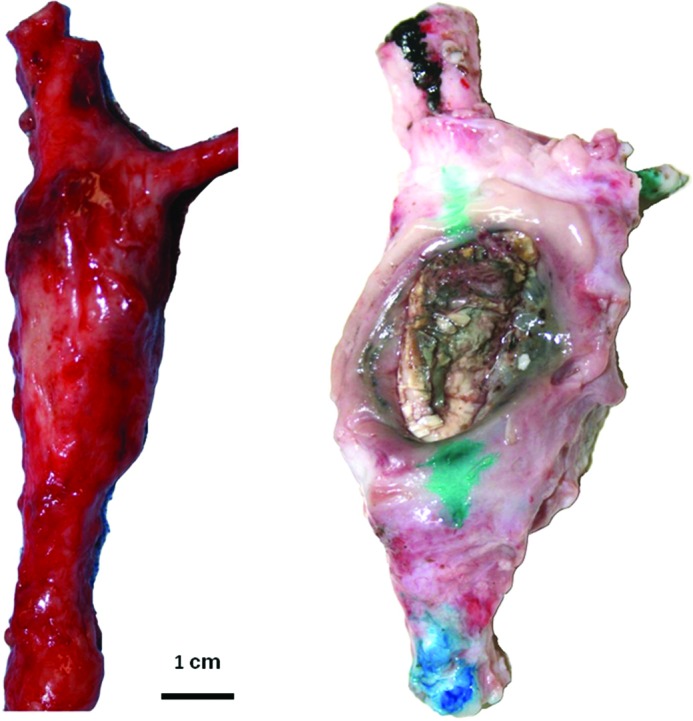
Postmortem photographs of infrarenal abdominal aortic aneurysms in pigs at the site of laparoscopically delivered periaortic calcium chloride. Both pigs had angiotensin-II infusion and were fed an atherogenic diet. The aneurysmatic aorta on the left was excised at 6 weeks. The AAA on the right ruptured at 5 weeks.
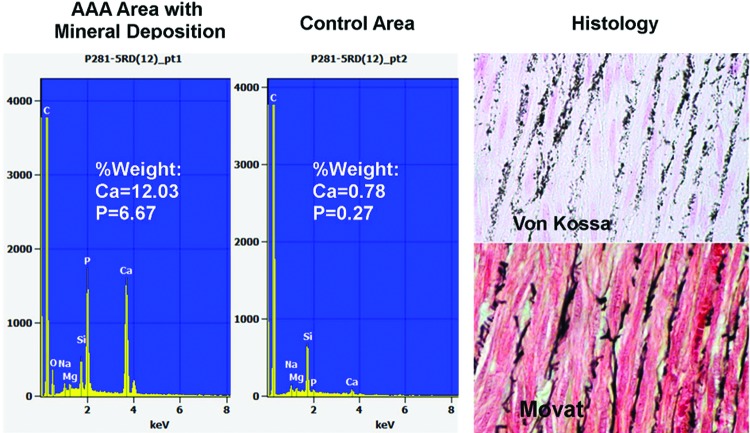
Left, Elemental analysis of porcine AAA by scanning electron microscopy (SEM) with electron dispersive spectrometery (EDS) showing calcium precipitates in the elastic lamellae. Right, top = Von Kossa-stained section showing calcium precipitates within the medial elastica as additionally confirmed with Movat pentachrome (bottom) that stains elastica black.
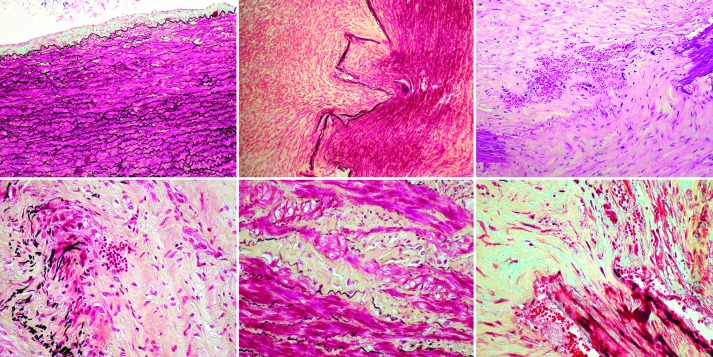
Infrarenal porcine abdominal aorta 4 weeks after laparoscopically delivered periarterial CaCl2 and angiotensin-II infusion by osmotic minipump inserted retroperitoneally by laparoscopy on the background of a 1-month high cholesterol, high fat diet. Top left, Relatively normal area adjacent to the site of calcium application (except for mild intimal hyperplasia). The remaining sections are from the site of aneurysm formation. Top middle, Marked disruption of the media with extensive fibromuscular hyperplasia (Movat). Top right, Transmedial disruption with fragmented elastica, neovascularization, RBC extravasation (H&E). Bottom left, Marked fragmentation of the elastic lamellae with infiltration of inflammatory cells including giant cells, some of which can be seen engulfing fragmented elastica (Movat). Bottom middle, Injury and depletion of smooth muscle cells with replacement by intercellular matrix (yellow) (Movat). Bottom right, Marked disruption of the media with fibrous tissue proliferation, neovascularization, and intramural extravasation of red blood cells (Movat).
Similar articles
-
Animal models of abdominal aortic aneurysm and their role in furthering management of human disease.Cardiovasc Pathol. 2011 Mar-Apr;20(2):114-23. doi: 10.1016/j.carpath.2010.01.001. Epub 2010 Feb 4. Cardiovasc Pathol. 2011. PMID: 20133168 Review.
-
Murine aortic aneurysm produced by periarterial application of calcium chloride.J Surg Res. 2001 Aug;99(2):371-6. doi: 10.1006/jsre.2001.6207. J Surg Res. 2001. PMID: 11469913
-
Endovascular model of abdominal aortic aneurysm induction in swine.Vasc Med. 2014 Jun;19(3):167-174. doi: 10.1177/1358863X14534006. Epub 2014 May 30. Vasc Med. 2014. PMID: 24879711
-
Different long-term outcomes of abdominal aortic aneurysm and intracranial aneurysm models: hemodynamic change may also play an essential role in the initiation and progression of abdominal aortic aneurysm in rabbits.Cell Biochem Biophys. 2014 Nov;70(2):819-22. doi: 10.1007/s12013-014-9985-5. Cell Biochem Biophys. 2014. PMID: 24801772
-
Recent Advances in the Development of Experimental Animal Models Mimicking Human Aortic Aneurysms.Vasc Specialist Int. 2015 Mar;31(1):1-10. doi: 10.5758/vsi.2015.31.1.1. Epub 2015 Mar 31. Vasc Specialist Int. 2015. PMID: 26217637 Free PMC article. Review.
Cited by
-
Computational Fluid Dynamics of Vascular Disease in Animal Models.J Biomech Eng. 2018 Aug 1;140(8):0808011-08080114. doi: 10.1115/1.4039678. J Biomech Eng. 2018. PMID: 29570754 Free PMC article. Review.
-
Abdominal Aortic Aneurysm: Evolving Controversies and Uncertainties.Int J Angiol. 2018 Jun;27(2):58-80. doi: 10.1055/s-0038-1657771. Epub 2018 May 29. Int J Angiol. 2018. PMID: 29896039 Free PMC article. Review.
-
Thrombin-Fibrinogen In Vitro Flow Model of Thrombus Growth in Cerebral Aneurysms.TH Open. 2021 May 12;5(2):e155-e162. doi: 10.1055/s-0041-1728790. eCollection 2021 Apr. TH Open. 2021. PMID: 34007954 Free PMC article.
-
Translating mouse models of abdominal aortic aneurysm to the translational needs of vascular surgery.JVS Vasc Sci. 2021 Mar 3;2:219-234. doi: 10.1016/j.jvssci.2021.01.002. eCollection 2021. JVS Vasc Sci. 2021. PMID: 34778850 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources