

Type B Aortic Dissection: A Review of Prognostic Factors and Meta-analysis of Treatment Options
- PMID: 26798745
- PMCID: PMC4682679
- DOI: 10.12945/j.aorta.2014.14-040
Type B Aortic Dissection: A Review of Prognostic Factors and Meta-analysis of Treatment Options
Abstract
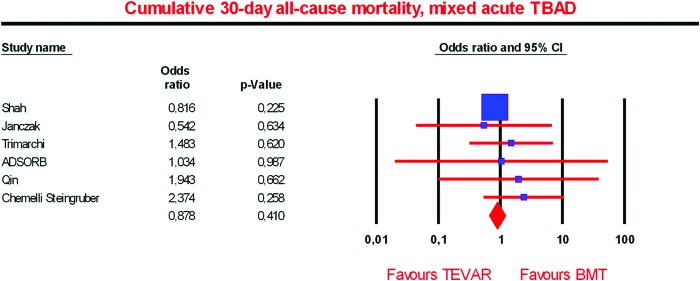
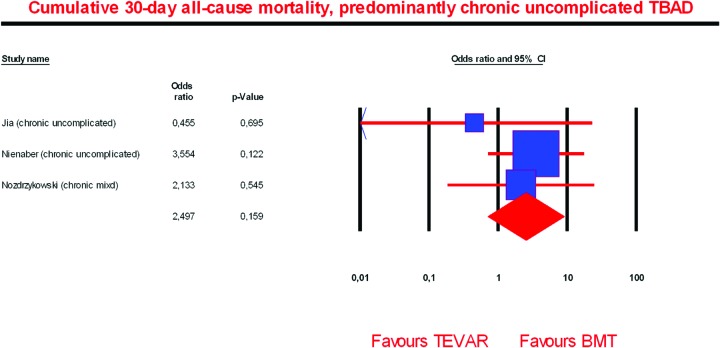
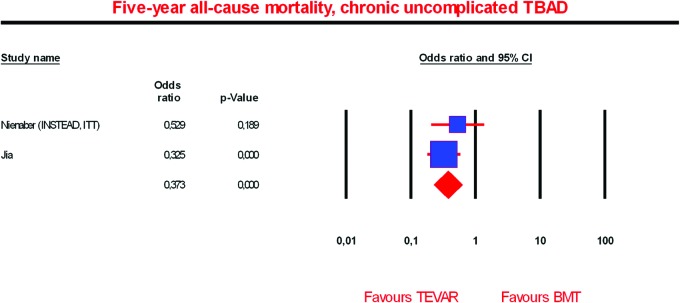
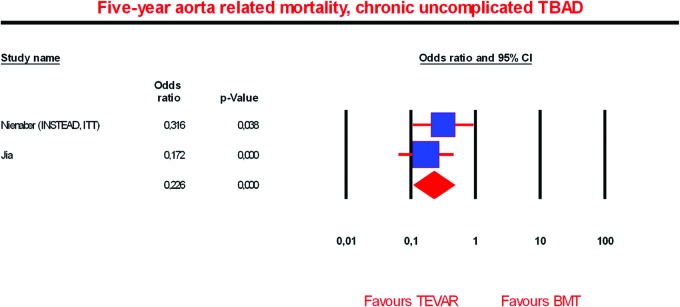
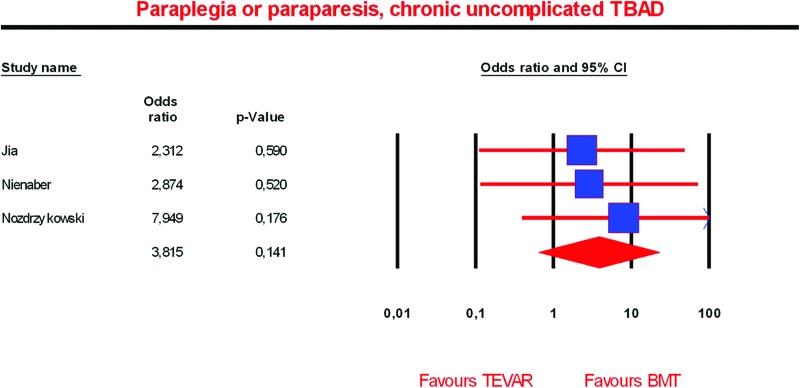
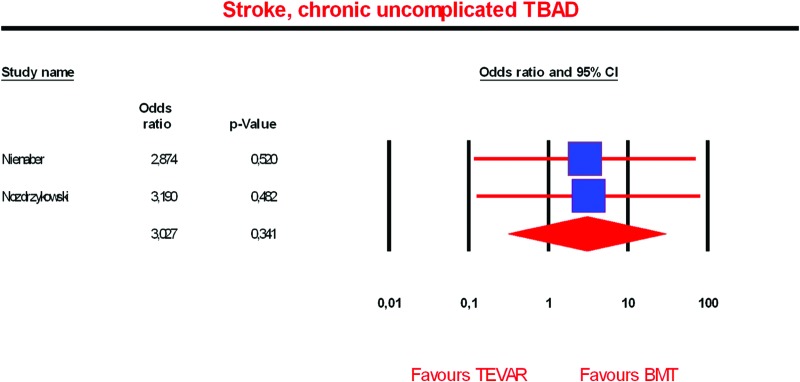
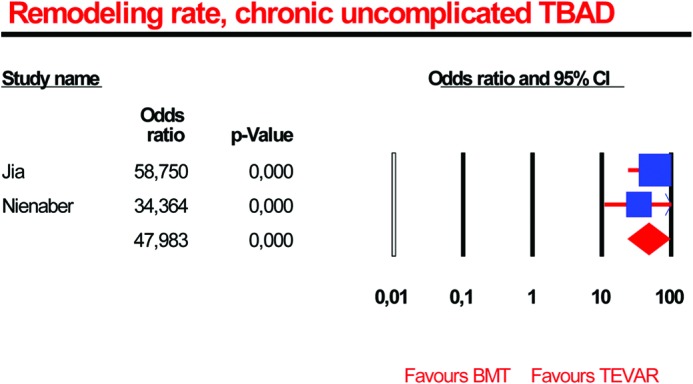
According to international guidelines, stable patients with uncomplicated Type B aortic dissection (TBAD) should receive optimal medical treatment. Despite adequate antihypertensive therapy, the long-term prognosis of these patients is characterized by a significant aortic aneurysm formation in 25-30% within four years, and survival rates from 50 to 80% at five years and 30 to 60% at 10 years. In a prospective randomized trial, preemptive thoracic endovascular aortic repair (TEVAR) in patients with chronic uncomplicated TBAD was associated with an excess early mortality (due to periprocedural hazards), but the procedure showed its benefit in prevention of aortic-specific mortality at five years of follow-up. However, preemptive TEVAR may not be the treatment of choice in all patients with uncomplicated TBAD because of the inherent periprocedural complications like stroke, paraparesis, and death, as well as stent graft-induced complications (i.e., retrograde dissection or endoleaks). Thus, the TEVAR-related deaths and complications (especially paraplegia and stroke) raise concerns that moderate the better survival with TEVAR at five years. By timely identification of those patients prone for developing complications, early intervention, preferably in the subacute or early chronic phase, may improve the overall long-term outcome for these patients. Therefore, early detectable and reliable prognostic factors for adverse events are essential to stratify patients who can be treated medically and those who will benefit from rigorous follow-up and, in the long-term, from timely, or even prophylactic, TEVAR. Several studies have identified prognostic factors in TBAD such as aortic diameter, partial false lumen thrombosis, false lumen thickness, and location of the primary entry tear. Combining these clinical and radiological predictors may be essential to implement a patient-specific approach designed to intervene only in those patients who are at high risk of developing complications to improve the long-term outcomes of patients with uncomplicated Type B aortic dissection.
Keywords: Endovascular; Thoracic aorta; Type B aortic dissection.
Figures
References
-
- Olsson C, Thelin S, Ståhle E, Ekbom A, Granath F. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation. 2006;114:2611–2618. 10.1161/CIRCULATIONAHA.106.630400 - DOI - PubMed
-
- Carpenter SW, Kodolitsch YV, Debus ES, Wipper S, Tsilimparis N, Larena-Avellaneda A, et al. Acute aortic syndromes: definition, prognosis and treatment options. J Cardiovasc Surg (Torino). 2014;55(2 Suppl 1):133–144. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources