

Maximum Diameter of Native Abdominal Aortic Aneurysm Measured by Angio-Computed Tomography: Reproducibility and Lack of Consensus Impacts on Clinical Decisions
- PMID: 26798757
- PMCID: PMC4686349
- DOI: 10.12945/j.aorta.2015.14-059
Maximum Diameter of Native Abdominal Aortic Aneurysm Measured by Angio-Computed Tomography: Reproducibility and Lack of Consensus Impacts on Clinical Decisions
Abstract
Background: Computed tomography angiography (CTA) is the reference technique for the measurement of native maximum abdominal aortic aneurysm (AAA) diameter when surgery is being considered. However, there is a wide choice available for the methodology of maximum AAA diameter measurement on CTA, and to date, no consensus has been reached on which method is best. We analyzed clinical decisions based on these various measures of native maximum AAA diameter with CTA, then analyzed their reproducibility and identified the method of measurement yielding the highest agreement in terms of patient management.
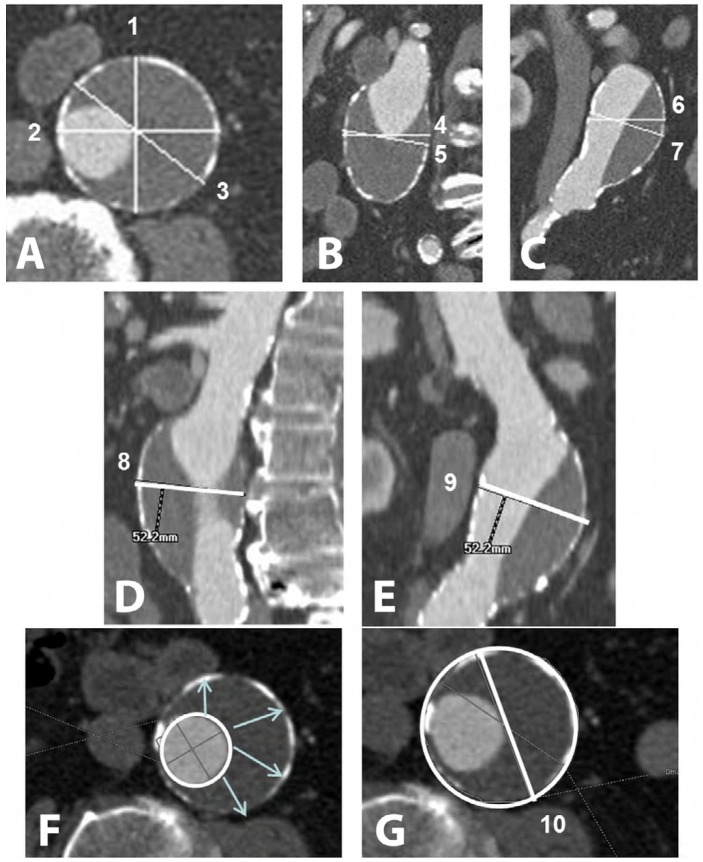
Materials and methods: Three sets of measures in 46 native AAA were obtained, double-blind by three radiologists (J, S, V) on orthogonal planes, curved multiplanar reconstructions, and semi-automated-software, based on the AAA-lumen centerline. From each set, the clinical decision was recorded as follows: "Follow-up" (if all diameters <50 mm), "ambiguous" (if at least one diameter <50 mm AND at least one ≥50 mm) or "Surgery " (if all diameters ≥50 mm). Intra- and interobserver agreements in clinical decisions were compared using the weighted Kappa coefficient.
Results: Clinical decisions varied according to the measurement sets used by each observer, and according to intra and interobserver (lecture#1) reproducibility. Based on the first reading of each observer, the number of AAA proposed for surgery ranged from 11 to 24 for J, 5 to 20 for S, and 15 to 23 for V. The rate of AAAs classified as "ambiguous" varied from 11% (5/46) to 37% (17/46). The semi-automated method yielded very good intraand interobserver agreements in clinical decisions in all comparisons (Kappa range 0.83-1.00).
Conclusion: The semi-automated method seems to be appropriate for native AAA maximum diameter measurement on CTA. In the absence of AAA outer-wallbased software more robust for complex AAA, clinical decisions might best be made with diameter values obtained using this technique.
Keywords: Abdominal aortic aneurysm; Computed tomography; Reproducibility.
Conflict of interest statement
Conflict of Interest:The authors have no conflict of interest relevant to this publication.
Figures
References
-
- Brewster DC, Cronenwett JL, Hallett JW Jr, Johnston KW, Krupski WC, Matsumura JS. . Joint Council of the American Association for Vascular Surgery and Society for Vascular Surgery. Guidelines for the treatment of abdominal aortic aneurysms. Report of a subcommittee of the Joint Council of the American Association for Vascular Surgery and Society for Vascular Surgery. J Vasc Surg. 2003;37:1106-1117. DOI: 10.1067/mva.2003.363 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources