

Actigraph measures discriminate pediatric bipolar disorder from attention-deficit/hyperactivity disorder and typically developing controls
- PMID: 26799153
- PMCID: PMC4873411
- DOI: 10.1111/jcpp.12520
Actigraph measures discriminate pediatric bipolar disorder from attention-deficit/hyperactivity disorder and typically developing controls
Abstract
Background: Distinguishing pediatric bipolar disorder (BD) from attention-deficit hyperactivity disorder (ADHD) can be challenging. Hyperactivity is a core feature of both disorders, but severely disturbed sleep and circadian dysregulation are more characteristic of BD, at least in adults. We tested the hypothesis that objective measures of activity, sleep, and circadian rhythms would help differentiate pediatric subjects with BD from ADHD and typically developing controls.
Methods: Unmedicated youths (N = 155, 97 males, age 5-18) were diagnosed using DSM-IV criteria with Kiddie-SADS PL/E. BD youths (n = 48) were compared to typically developing controls (n = 42) and children with ADHD (n = 44) or ADHD plus comorbid depressive disorders (n = 21). Three-to-five days of minute-to-minute belt-worn actigraph data (Ambulatory Monitoring Inc.), collected during the school week, were processed to yield 28 metrics per subject, and assessed for group differences with analysis of covariance. Cross-validated machine learning algorithms were used to determine the predictive accuracy of a four-parameter model, with measures reflecting sleep, hyperactivity, and circadian dysregulation, plus Indic's bipolar vulnerability index (VI).
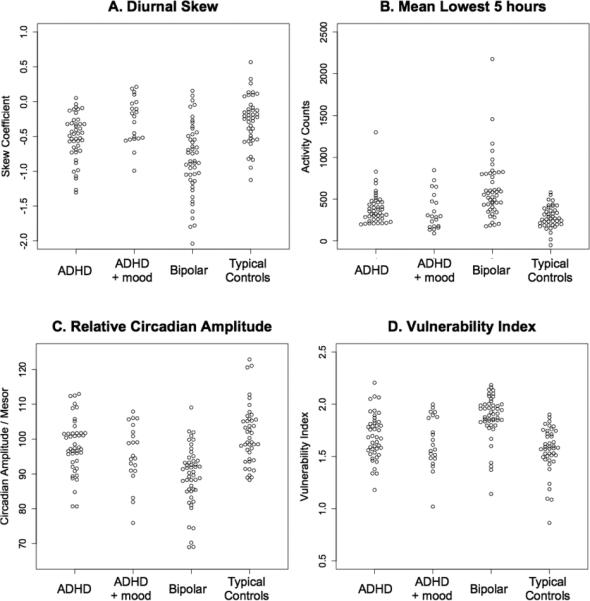
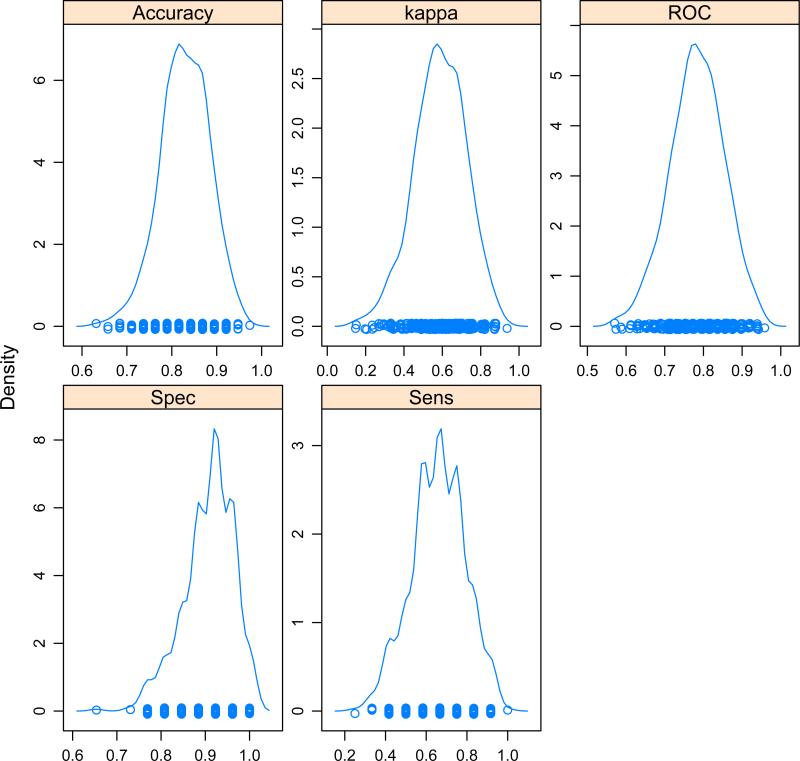
Results: There were prominent group differences in several activity measures, notably mean 5 lowest hours of activity, skewness of diurnal activity, relative circadian amplitude, and VI. A predictive support vector machine model discriminated bipolar from non-bipolar with mean accuracy of 83.1 ± 5.4%, ROC area of 0.781 ± 0.071, kappa of 0.587 ± 0.136, specificity of 91.7 ± 5.3%, and sensitivity of 64.4 ± 13.6%.
Conclusions: Objective measures of sleep, circadian rhythmicity, and hyperactivity were abnormal in BD. Wearable sensor technology may provide bio-behavioral markers that can help differentiate children with BD from ADHD and healthy controls.
Keywords: ADHD; Actigraphy; bipolar disorder; child; circadian rhythms; sleep.
© 2016 Association for Child and Adolescent Mental Health.
Figures
References
-
- ACEBO C, SADEH A, SEIFER R, TZISCHINSKY O, WOLFSON AR, HAFER A, CARSKADON MA. Estimating sleep patterns with activity monitoring in children and adolescents: how many nights are necessary for reliable measures? Sleep. 1999;22:95–103. - PubMed
-
- AMERICAN PSYCHIATRIC ASSOCIATION . Diagnostic and statistical manual of mental disorders. American Psychiatric Publishing; Arlington, VA: 2013.
-
- ANGST J, GAMMA A, BENAZZI F, AJDACIC V, EICH D, ROSSLER W. Toward a re-definition of subthreshold bipolarity: epidemiology and proposed criteria for bipolar-II, minor bipolar disorders and hypomania. J Affect Disord. 2003;73:133–146. - PubMed
-
- ARNS M, KENEMANS JL. Neurofeedback in ADHD and insomnia: vigilance stabilization through sleep spindles and circadian networks. Neurosci Biobehav Rev. 2014;44:183–194. - PubMed
-
- AXELSON DA, BIRMAHER B, STROBER MA, GOLDSTEIN BI, HA W, GILL MK, GOLDSTEIN TR, YEN S, HOWER H, HUNT JI, LIAO F, IYENGAR S, DICKSTEIN D, KIM E, RYAN ND, FRANKEL E, KELLER MB. Course of subthreshold bipolar disorder in youth: diagnostic progression from bipolar disorder not otherwise specified. J Am Acad Child Adolesc Psychiatry. 2011;50:1001–1016. e1003. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
