

Infection in Health Personnel with High and Low Levels of Exposure in a Hospital Setting during the H1N1 2009 Influenza A Pandemic
- PMID: 26799564
- PMCID: PMC4723060
- DOI: 10.1371/journal.pone.0147271
Infection in Health Personnel with High and Low Levels of Exposure in a Hospital Setting during the H1N1 2009 Influenza A Pandemic
Abstract
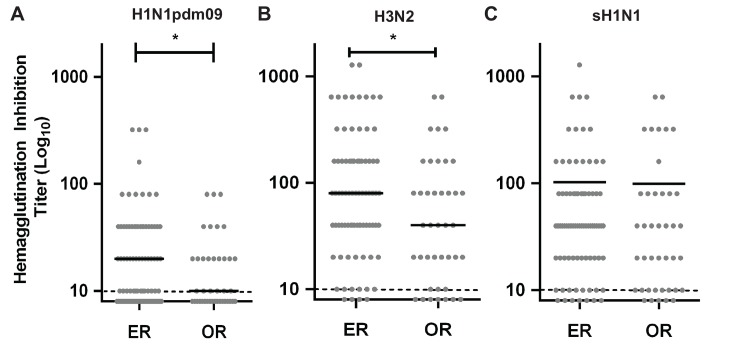
A novel H1N1 influenza A virus caused the first pandemic of the 21st century in 2009. Hospitals had an increased demand of health consultations, that made it difficult to estimate the incidence of infection in hospital personnel due to asymptomatic presentations and the under notification of cases. To estimate and compare the rate of exposure of high versus low risk health personnel to 2009 pandemic H1N1 (H1N1pdm2009) influenza A virus in a University Hospital in Chile, we performed a comparative and prospective study. Serum samples were obtained from 117 individuals that worked in the emergency room (ER) and the operating room (OR) during the peak of the pandemic. Antibody titers were determined by the hemagglutination inhibition (HI) assay. Of the samples analyzed, 65% were workers at the ER and 35% at the OR. Of the total number of the subjects tested, 29.1% were seropositive. One out of 3 (36.8%) workers at the ER had positive HI titers, meanwhile only 1 out of 7 (14.6%) workers from the OR was seropositive to the virus. The possibility of being infected in the ER as compared to the OR was 3.4 times greater (OR 3.4; CI 95%, 1.27-9.1), and the individuals of the ER had almost twice as much antibody titers against H1N1pdm2009 than the personnel in the OR, suggesting the potential of more than one exposure to the virus. Of the 34 seropositive subjects, 12 (35.3%) did not develop influenza like illness, including 2 non-clinical personnel involved in direct contact with patients at the ER. Considering the estimated population attack rate in Chile of 13%, both groups presented a higher exposure and seropositive rate than the general population, with ER personnel showing greater risk of infection and a significantly higher level of antibodies. This data provide a strong rationale to design improved control measures aimed at all the hospital personnel, including those coming into contact with the patients prior to triage, to prevent the propagation and transmission of respiratory viruses, particularly during a pandemic outbreak.
Conflict of interest statement
Figures
References
-
- Wise ME, De Perio M, Halpin J, Jhung M, Magill S, Black SR, et al. Transmission of pandemic (H1N1) 2009 influenza to healthcare personnel in the United States. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America. 2011;52 Suppl 1:S198–204. 10.1093/cid/ciq038 . - DOI - PubMed
-
- Chan YJ, Lee CL, Hwang SJ, Fung CP, Wang FD, Yen DH, et al. Seroprevalence of antibodies to pandemic (H1N1) 2009 influenza virus among hospital staff in a medical center in Taiwan. Journal of the Chinese Medical Association: JCMA. 2010;73(2):62–6. 10.1016/S1726-4901(10)70003-4 . - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
