

Interactions and relevance of blast percentage and treatment strategy among younger and older patients with acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS)
- PMID: 26799610
- PMCID: PMC5486407
- DOI: 10.1002/ajh.24252
Interactions and relevance of blast percentage and treatment strategy among younger and older patients with acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS)
Abstract
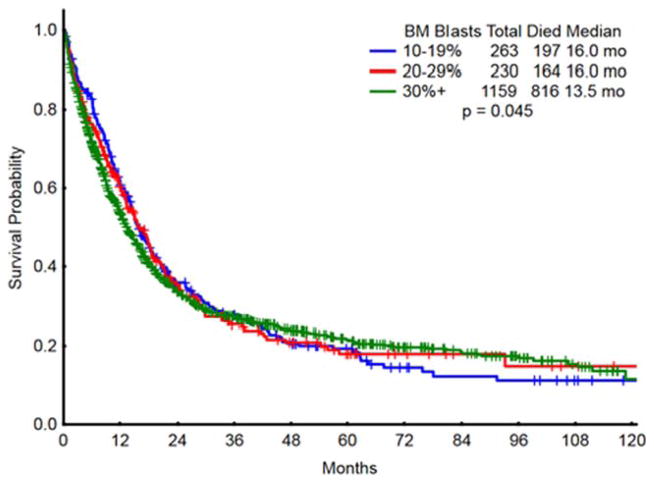
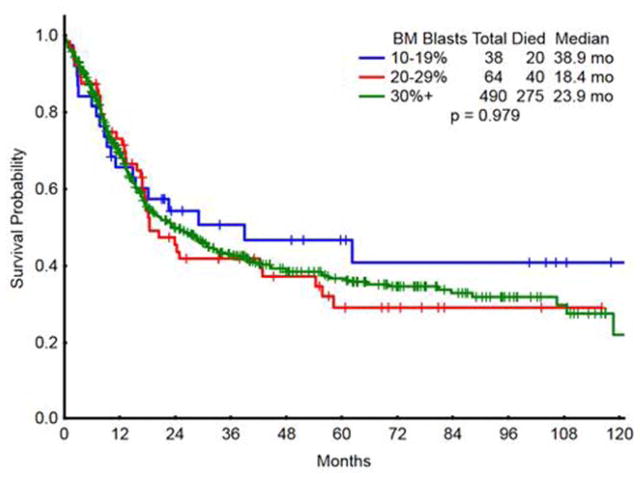
Acute myeloid leukemia (AML) is defined as ≥20% myeloblasts, representing a change from original guidelines where ≤30% blasts were considered as myelodysplastic syndromes (MDS), and 20-29% blasts classified as refractory anemia with excess blasts in transformation (RAEB-T). Whether the diagnostic bone marrow blast percentage has current value with regards to patient prognostication or identification of optimal treatment strategies is unclear. We retrospectively studied 1652 treatment-naïve adults with MDS or AML and ≥10% blasts from January 2000 to April 2014. Patients with 20-29% blasts were more similar to MDS patients in terms of advanced age, increased frequency of poor-risk cytogenetics, lower WBC count, and less frequent NPM1 and FLT3-ITD mutations. Median overall survival of MDS and RAEB-T were similar, 16.0 and 16.0 months, compared to 13.5 months for AML with ≥30% blasts (P = 0.045). Multivariate analysis showed inferior survival with increased age (HR 1.81 age 60-69, HR 2.68 age ≥70, P < 0.0005); poor-risk cytogenetics (HR 2.25, P < 0.0005); therapy-related disease (HR 1.44, P < 0.0005); and markers of proliferative disease including WBC ≥25 × 10(9) /L (HR 1.35, P = 0.0003), elevated LDH count (HR 1.24, P = 0.0015), and peripheral blasts (HR 1.25, P = 0.004). Among younger patients (≤60 years), intensive AML-type therapy resulted in similar outcomes regardless of blast percentage, suggesting this to be optimal therapy in this context. Among older patients (≥70 years), patients with 20-29% blasts had similar outcomes to patients with <20% blasts, and better than those with ≥30% blasts. In addition, among older patients, epigenetic therapy provided at least equivalent outcome to intensive chemotherapy.
© 2015 Wiley Periodicals, Inc.
Figures
Similar articles
-
Clinical and biological characteristics of acute myeloid leukemia with 20-29% blasts: a retrospective single-center study.Leuk Lymphoma. 2019 May;60(5):1136-1145. doi: 10.1080/10428194.2018.1515938. Epub 2018 Oct 10. Leuk Lymphoma. 2019. PMID: 30301399
-
Epigenetic priming with decitabine followed by low dose idarubicin and cytarabine in acute myeloid leukemia evolving from myelodysplastic syndromes and higher-risk myelodysplastic syndromes: a prospective multicenter single-arm trial.Hematol Oncol. 2020 Oct;38(4):531-540. doi: 10.1002/hon.2755. Epub 2020 Jun 24. Hematol Oncol. 2020. PMID: 32469434
-
De novo acute myeloid leukemia with 20-29% blasts is less aggressive than acute myeloid leukemia with ≥30% blasts in older adults: a Bone Marrow Pathology Group study.Am J Hematol. 2014 Nov;89(11):E193-9. doi: 10.1002/ajh.23808. Epub 2014 Jul 31. Am J Hematol. 2014. PMID: 25042343
-
Myelodysplastic syndrome in children: differentiation from acute myeloid leukemia with a low blast count.Leukemia. 1997 Feb;11(2):206-11. doi: 10.1038/sj.leu.2400558. Leukemia. 1997. PMID: 9009082 Review.
-
[Myelodysplastic syndromes (MDS). Aspects of hematopathologic diagnosis].Pathologe. 2000 Jan;21(1):1-15. doi: 10.1007/s002920050001. Pathologe. 2000. PMID: 10663664 Review. German.
Cited by
-
Distinguishing AML from MDS: a fixed blast percentage may no longer be optimal.Blood. 2022 Jan 20;139(3):323-332. doi: 10.1182/blood.2021011304. Blood. 2022. PMID: 34111285 Free PMC article.
-
Olive leaves extract alleviates inflammation and modifies the intrinsic apoptotic signal in the leukemic bone marrow.Front Immunol. 2023 Jan 19;13:1054186. doi: 10.3389/fimmu.2022.1054186. eCollection 2022. Front Immunol. 2023. PMID: 36741365 Free PMC article.
-
Machine Learning to Predict Risk of Relapse Using Cytologic Image Markers in Patients With Acute Myeloid Leukemia Posthematopoietic Cell Transplantation.JCO Clin Cancer Inform. 2022 May;6:e2100156. doi: 10.1200/CCI.21.00156. JCO Clin Cancer Inform. 2022. PMID: 35522898 Free PMC article. Clinical Trial.
-
Severe atypical herpes zoster as an initial symptom of fatal myelodysplastic syndrome with refractory anemia and blast excess (RAEB II).Clin Cosmet Investig Dermatol. 2017 May 18;10:195-198. doi: 10.2147/CCID.S133966. eCollection 2017. Clin Cosmet Investig Dermatol. 2017. PMID: 28652792 Free PMC article.
-
Acute Myeloid Leukemia: 2025 Update on Diagnosis, Risk-Stratification, and Management.Am J Hematol. 2025 May;100(5):860-891. doi: 10.1002/ajh.27625. Epub 2025 Feb 12. Am J Hematol. 2025. PMID: 39936576 Free PMC article. Review.
References
-
- Bennett JM, Catovsky D, Daniel MT, et al. Proposals for the classification of the acute leukaemias. French-American-British (FAB) cooperative group. Br J Haematol. 1976;33:451–458. - PubMed
-
- Greenberg P, Cox C, LeBeau MM, et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood. 1997;89:2079–2088. Epub 1997/03/15. eng. - PubMed
-
- Vardiman JW, Harris NL, Brunning RD. The World Health Organization (WHO) classification of the myeloid neoplasms. Blood. 2002;100:2292–2302. - PubMed
-
- Bernstein SH, Brunetto VL, Davey FR, et al. Acute myeloid leukemia-type chemotherapy for newly diagnosed patients without antecedent cytopenias having myelodysplastic syndrome as defined by French-American-British criteria: a Cancer and Leukemia Group B Study. J Clin Oncol. 1996;14:2486–2494. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous