

Treatment options for infections caused by carbapenem-resistant Enterobacteriaceae: can we apply "precision medicine" to antimicrobial chemotherapy?
- PMID: 26799840
- PMCID: PMC4970584
- DOI: 10.1517/14656566.2016.1145658
Treatment options for infections caused by carbapenem-resistant Enterobacteriaceae: can we apply "precision medicine" to antimicrobial chemotherapy?
Abstract
Introduction: For the past three decades, carbapenems played a central role in our antibiotic armamentarium, trusted to effectively treat infections caused by drug-resistant bacteria. The utility of this class of antibiotics has been compromised by the emergence of resistance especially among Enterobacteriaceae.
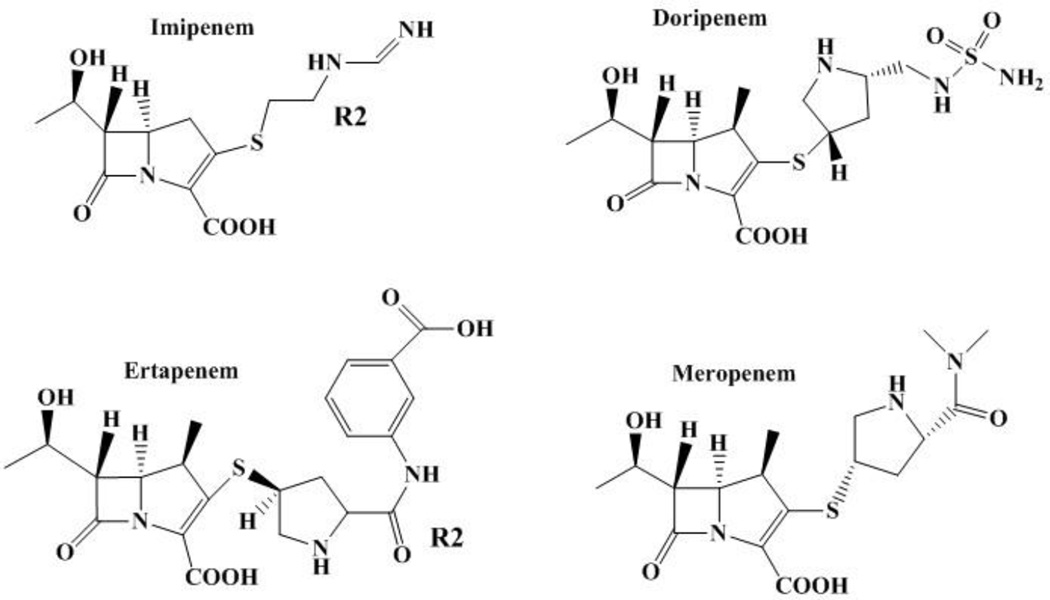
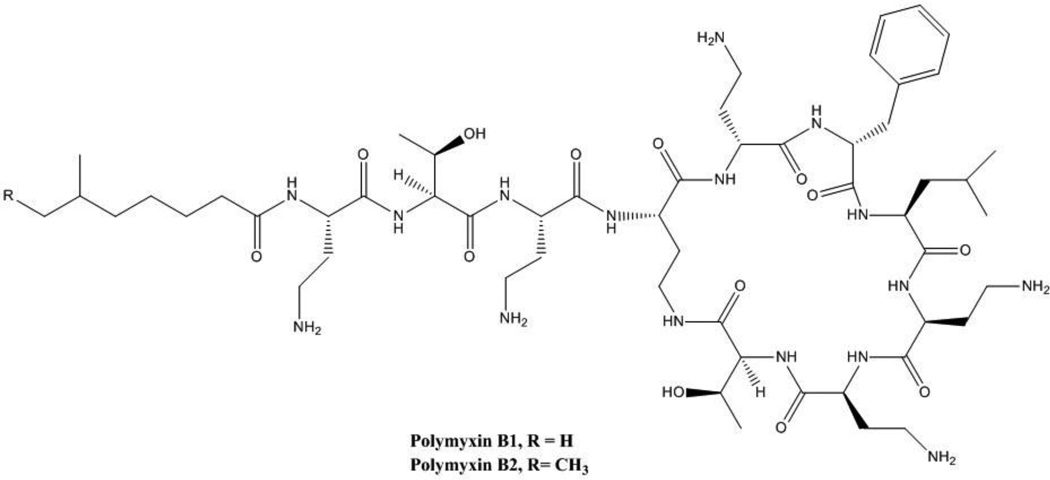
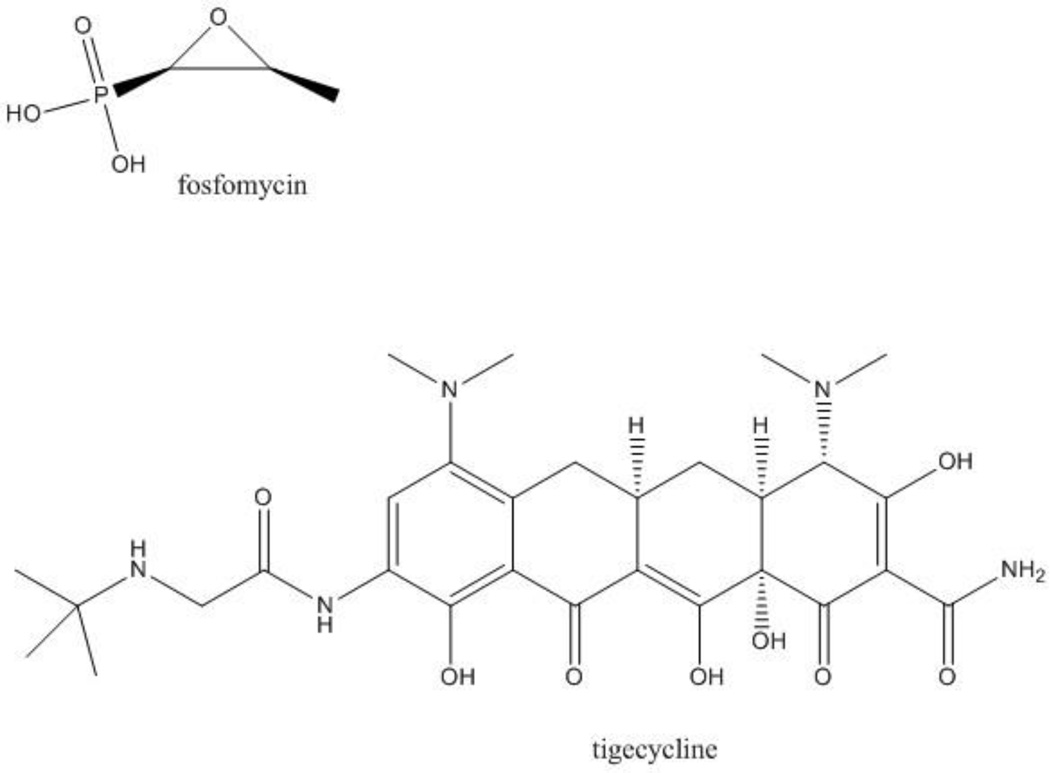
Areas covered: We review the current mainstays of pharmacotherapy against infections caused by carbapenem-resistant Enterobacteriaceae (CRE) including tigecycline, aminoglycosides, and rediscovered 'old' antibiotics such as fosfomycin and polymyxins, and discuss their efficacy and potential toxicity. We also summarize the contemporary clinical experience treating CRE infections with antibiotic combination therapy. Finally, we discuss ceftazidime/avibactam and imipenem/relebactam, containing a new generation of beta-lactamase inhibitors, which may offer alternatives to treat CRE infections. We critically evaluate the published literature, identify relevant clinical trials and review documents submitted to the United States Food and Drug Administration.
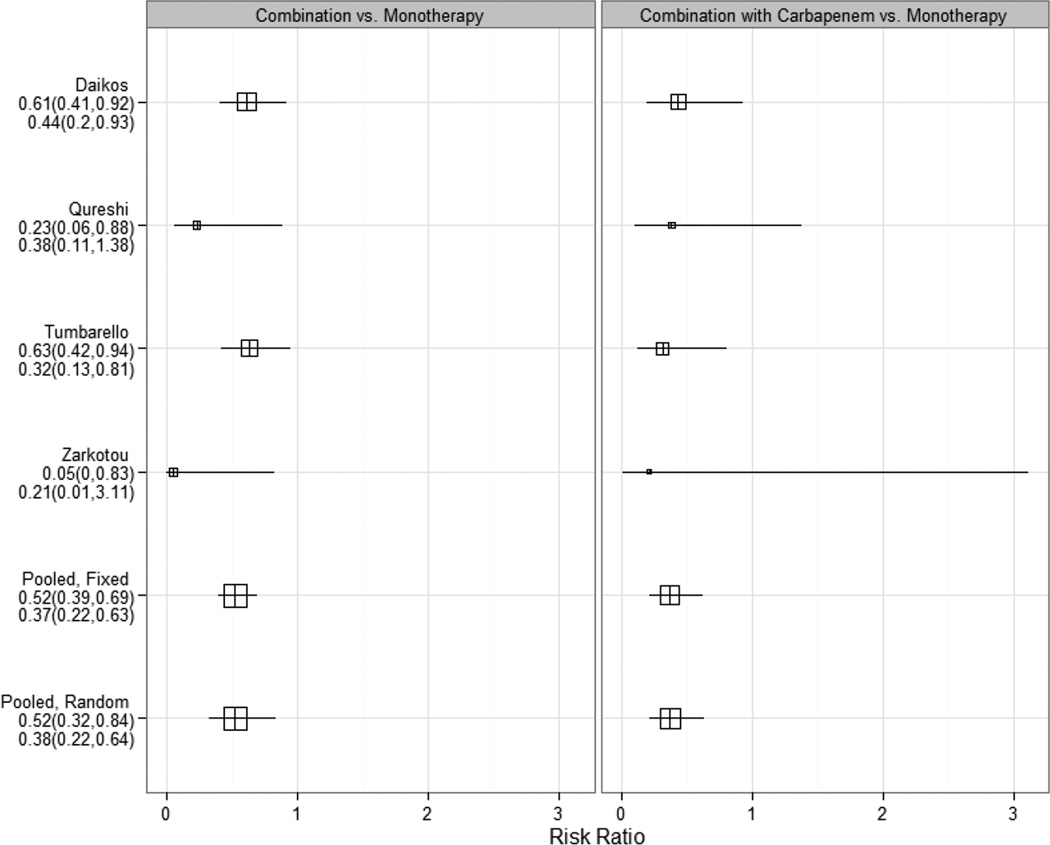
Expert opinion: Defining the molecular mechanisms of resistance and applying insights about pharmacodynamic and pharmacokinetic properties of antibiotics, in order to maximize the impact of old and new therapeutic approaches should be the new paradigm in treating infections caused by CRE. A concerted effort is needed to carry out high-quality clinical trials that: i) establish the superiority of combination therapy vs. monotherapy; ii) confirm the role of novel beta-lactam/beta-lactamase inhibitor combinations as therapy against KPC- and OXA-48 producing Enterobacteriaceae; and, iii) evaluate new antibiotics active against CRE as they are introduced into the clinic.
Keywords: Enterobacteriaceae; beta-lactamase inhibitors; carbapenems; drug combinations; drug resistance; multiple.
Conflict of interest statement
The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Figures
References
-
- Kahan JS, Kahan FM, Goegelman R, et al. Thienamycin, a new beta-lactam antibiotic. I. Discovery, taxonomy, isolation and physical properties. J Antibiot (Tokyo) 1979;32(1):1–12. - PubMed
-
- Kahan JSK, F M, Goegelman R, Currie SA, Jackson M, Stapley EO, Miller TW, Miller AK, Hendlin D, Mochales S, Hernandez S, Woodruff HS. Abstract XVI. Interscience Conference on Antimicrobial Agents and Chemotherapy; American Society for Microbiology; Chicago. 1976.
-
- Romagnoli MF, Fu KP, Neu HC. The antibacterial activity of thienamycin against multiresistant bacteria-comparison with beta-lactamase stable compounds. J Antimicrob Chemother. 1980;6(5):601–606. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous