

The existence of standard-biased mortality ratios due to death certificate misclassification - a simulation study based on a true story
- PMID: 26801235
- PMCID: PMC4722668
- DOI: 10.1186/s12874-016-0112-8
The existence of standard-biased mortality ratios due to death certificate misclassification - a simulation study based on a true story
Abstract
Background: Mortality statistics are used to compare health status of populations; optimally, they base on individual death certificates. However, determining cause of death is error-prone. E.g. cardiovascular disease (CVD) death determination is characterized by sensitivity (SE) and specificity (SP) lower than 85%. Furthermore, differential misclassification may be present in case of homogenous target populations. We investigate the bias of standardized mortality ratios (SMR), based on real-world data.
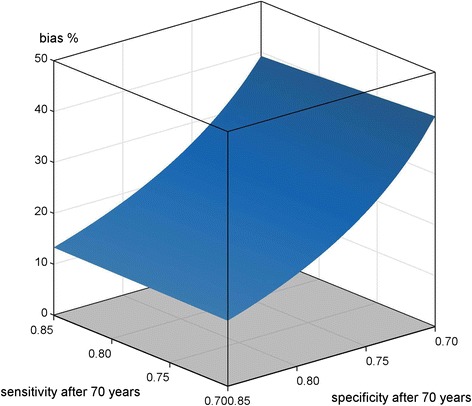
Methods: CVD mortality of 6378 ethnic German repatriates was assessed and the SMR calculated. Non-differential age-dependent misclassification was introduced into data by scenarios of equal SE and SP in a range of 0.7 to 0.85. The bias between originally reported and actual SMR was calculated for each pair of values. Additionally, four differential misclassification scenarios were simulated, reflecting two extreme scenarios of both quality criteria varied in the cohort but fixed to either higher or lower in the reference, and two scenarios of crossed criteria values.
Results: In case of non-differential misclassification the bias is always towards the null-hypothesis. The lowest bias was 13.5% (SE, SP = 0.85 constantly), the maximum bias was 40% (SP = 0.7). However, in case of differential misclassification the observed SMR can be on the wrong track. If SP is high but SE low in the cohort, negative bias up to -10% can occur. In case SE is low but SP is high in the reference, the bias remains always positive. In the opposite case plus SP is high in the cohort, the bias can reach -30%.
Conclusion: SMR values are always biased due to the diagnostic test character of death determination. In majority of epidemiological studies the bias should be towards the null-hypothesis (non-differential misclassification). However, caution is needed in case of differential misclassification, possibly experienced in studies on homogenous subgroups, and in large prospective cohorts with specifically trained personnel.
Figures




Similar articles
-
Patterns of bias due to differential misclassification by case-control status in a case-control study.Eur J Epidemiol. 2007;22(1):7-17. doi: 10.1007/s10654-006-9078-x. Epub 2007 Jan 17. Eur J Epidemiol. 2007. PMID: 17225958
-
The effect of misclassification error on risk estimation in case-control studies.Rev Bras Epidemiol. 2015 Apr-Jun;18(2):341-56. doi: 10.1590/1980-5497201500020005. Rev Bras Epidemiol. 2015. PMID: 26083507
-
Bias Implications of Outcome Misclassification in Observational Studies Evaluating Association Between Treatments and All-Cause or Cardiovascular Mortality Using Administrative Claims.J Am Heart Assoc. 2020 Sep;9(17):e016906. doi: 10.1161/JAHA.120.016906. Epub 2020 Aug 26. J Am Heart Assoc. 2020. PMID: 32844711 Free PMC article.
-
The impact of under and over-recording of cancer on death certificates in a competing risks analysis: a simulation study.Cancer Epidemiol. 2013 Feb;37(1):11-9. doi: 10.1016/j.canep.2012.08.012. Epub 2012 Sep 20. Cancer Epidemiol. 2013. PMID: 22999870 Review.
-
Effects of misclassification on estimates of relative risk in family history studies.Genet Epidemiol. 1999;16(4):368-81. doi: 10.1002/(SICI)1098-2272(1999)16:4<368::AID-GEPI4>3.0.CO;2-A. Genet Epidemiol. 1999. PMID: 10207718 Review.
Cited by
-
One-year mortality and years of potential life lost following bloodstream infection among adults: A nation-wide population based study.Lancet Reg Health Eur. 2022 Sep 17;23:100511. doi: 10.1016/j.lanepe.2022.100511. eCollection 2022 Dec. Lancet Reg Health Eur. 2022. PMID: 36158527 Free PMC article.
-
Marital status, household size, and lifestyle changes during the first COVID-19 pandemic: NIPPON DATA2010.PLoS One. 2023 Mar 27;18(3):e0283430. doi: 10.1371/journal.pone.0283430. eCollection 2023. PLoS One. 2023. PMID: 36972241 Free PMC article.
-
Suboptimal oral health and the risk of cardiovascular disease in the presence of competing death: a data linkage analysis.Can J Public Health. 2023 Feb;114(1):125-137. doi: 10.17269/s41997-022-00675-z. Epub 2022 Sep 6. Can J Public Health. 2023. PMID: 36068436 Free PMC article.
-
Cause-specific mortality in individuals with lymphoplasmacytic lymphoma/Waldenström macroglobulinaemia, 2000-2016.Br J Haematol. 2020 Jun;189(6):1107-1118. doi: 10.1111/bjh.16492. Epub 2020 Feb 23. Br J Haematol. 2020. PMID: 32090327 Free PMC article.
-
Mortality in women with a history of incarceration in Norway: a 20-year national cohort study.Int J Epidemiol. 2024 Feb 14;53(2):dyae032. doi: 10.1093/ije/dyae032. Int J Epidemiol. 2024. PMID: 38481122 Free PMC article.
References
-
- Phillips DE, AbouZahr C, Lopez AD, Mikkelsen L, de Savigny D, Lozano R, et al. Are well functioning civil registration and vital statistics systems associated with better health outcomes? [published online ahead of print May 2005]. Lancet. doi:10.1016/S0140-6736(15)60172-6 - PubMed
-
- Shibuya K, Gilmour S. Civil registration as a means to promote human security. [published online ahead of print May 2005]. Lancet. (doi:10.1016/S0140-6736(15)60765-6) - PubMed
-
- Kreienbrock L, Schach S. In: Epidemiologische Methoden. (German) 4. Moltmann UG, editor. Heidelberg: Spektrum Akademischer Verlag; 2005.
-
- Andersson P, Leppert J. Men of low socio-economic and educational level possess pronounced deficient knowledge about the risk factors related to coronary heart disease. J Cardiovasc Risk. 2001;8(6):371–377. - PubMed
-
- Mikkelsen L, Phillips DE, AbouZahr C, Setel PW, de Savigny D, Lozano R, et al. A global assessment of civil registration and vital statistics systems: monitoring data quality and progress. [published online ahead of print May 2005]. Lancet. doi:10.1016/S0140-6736(15)60171-4 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
