

Clinicopathological analysis in patients with neuroendocrine tumors that metastasized to the brain
- PMID: 26801624
- PMCID: PMC4724130
- DOI: 10.1186/s12885-015-1999-x
Clinicopathological analysis in patients with neuroendocrine tumors that metastasized to the brain
Abstract
Background: A neuroendocrine tumor (NET) can develop anywhere in the body, but is mainly found in the pancreas, gastrointestinal tract, and lungs. This report is a retrospective study of the clinicopathological features of NET patients with brain metastasis whose tissue diagnosis was made at our hospital.
Methods: Patients with brain metastasis evidenced by clinical records and images were accumulated among 302 patients in whom tissue diagnosis of NETs was made at our hospital between 2008 and 2013. In the patients, the primary lesion, pathological classification, pattern of metastasis, details of treatment, and outcomes were analyzed.
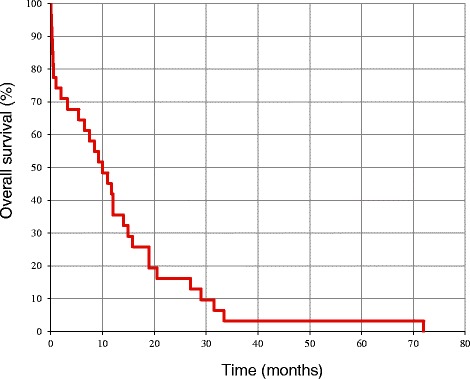
Results: Brain metastasis was observed in 31 patients (10.3%). The primary lesion was in the lungs in 26 patients (83.9%), and the mammary glands, esophagus, and uterus in 1 patient each. Primary lesions were unknown in 2 patients, including 1 patient in whom NETs were detected in the lymph nodes alone. Pathological classification of the primary lesion was NET Grade 2 (Ki-67: 3 to 20%) in 3 patients and neuroendocrine carcinoma (NEC, Ki-67: ≥ 21%) in 26 patients. The median period from onset of the primary lesion up to diagnosis of brain metastasis was 12.8 months, and the brain lesion preceded brain metastasis in 6 patients. Ten patients had a single metastasis whereas 21 patients had multiple metastases, but no characteristics were observed in their images. Brain metastasis was extirpated in 10 patients. Stereotactic radiotherapy alone was administered in 6 patients, and brain metastasis was favorably controlled in most of the patients with coadministration of cranial irradiation as appropriate. The median survival period from diagnosis of brain metastasis was 8.1 months, and the major cause of death was aggravation of the primary lesion or metastatic lesions in other organs.
Conclusion: Most of NET patients with brain metastasis showed the primary lesion of NEC in the lungs, and they had multiple metastases to the liver, lymph nodes, bones, and so forth at the time of diagnosis of brain metastasis. The guidelines for accurate diagnosis and treatment of NETs should be immediately established based on further analyses of NET patients with brain metastasis.
Figures




References
-
- Oberndorfer S. Karzinoide tumoren des dünndarms. Frankf Z Pathol. 1907;1:425–429.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
