

Global variations and time trends in the prevalence of childhood myopia, a systematic review and quantitative meta-analysis: implications for aetiology and early prevention
- PMID: 26802174
- PMCID: PMC4941141
- DOI: 10.1136/bjophthalmol-2015-307724
Global variations and time trends in the prevalence of childhood myopia, a systematic review and quantitative meta-analysis: implications for aetiology and early prevention
Abstract
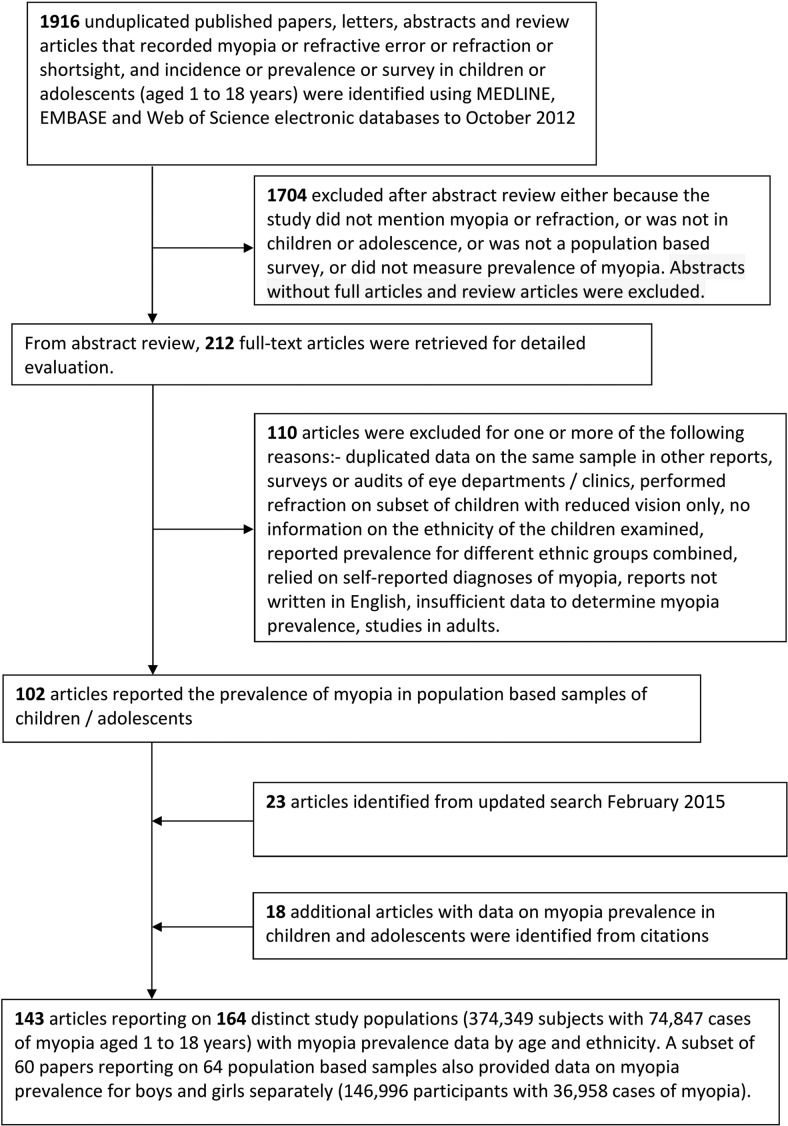
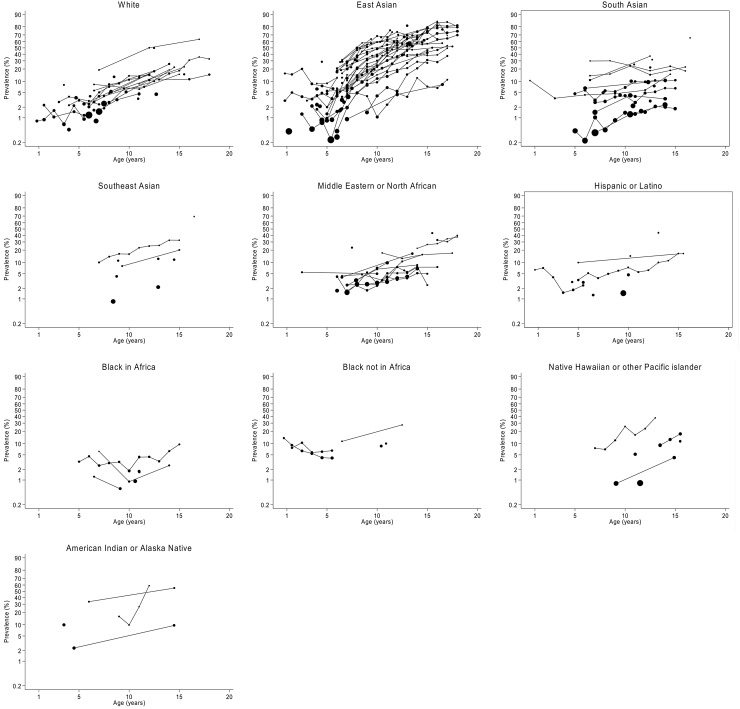
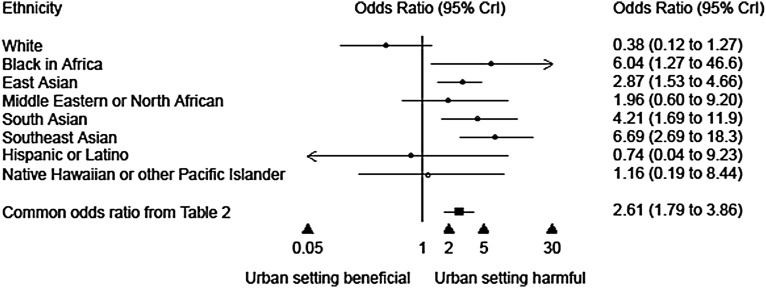
The aim of this review was to quantify the global variation in childhood myopia prevalence over time taking account of demographic and study design factors. A systematic review identified population-based surveys with estimates of childhood myopia prevalence published by February 2015. Multilevel binomial logistic regression of log odds of myopia was used to examine the association with age, gender, urban versus rural setting and survey year, among populations of different ethnic origins, adjusting for study design factors. 143 published articles (42 countries, 374 349 subjects aged 1-18 years, 74 847 myopia cases) were included. Increase in myopia prevalence with age varied by ethnicity. East Asians showed the highest prevalence, reaching 69% (95% credible intervals (CrI) 61% to 77%) at 15 years of age (86% among Singaporean-Chinese). Blacks in Africa had the lowest prevalence; 5.5% at 15 years (95% CrI 3% to 9%). Time trends in myopia prevalence over the last decade were small in whites, increased by 23% in East Asians, with a weaker increase among South Asians. Children from urban environments have 2.6 times the odds of myopia compared with those from rural environments. In whites and East Asians sex differences emerge at about 9 years of age; by late adolescence girls are twice as likely as boys to be myopic. Marked ethnic differences in age-specific prevalence of myopia exist. Rapid increases in myopia prevalence over time, particularly in East Asians, combined with a universally higher risk of myopia in urban settings, suggest that environmental factors play an important role in myopia development, which may offer scope for prevention.
Keywords: Child health (paediatrics); Epidemiology; Optics and Refraction; Public health.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical