

A novel device for accurate and efficient testing for vision-threatening diabetic retinopathy
- PMID: 26803474
- PMCID: PMC4853922
- DOI: 10.1016/j.jdiacomp.2015.12.005
A novel device for accurate and efficient testing for vision-threatening diabetic retinopathy
Abstract
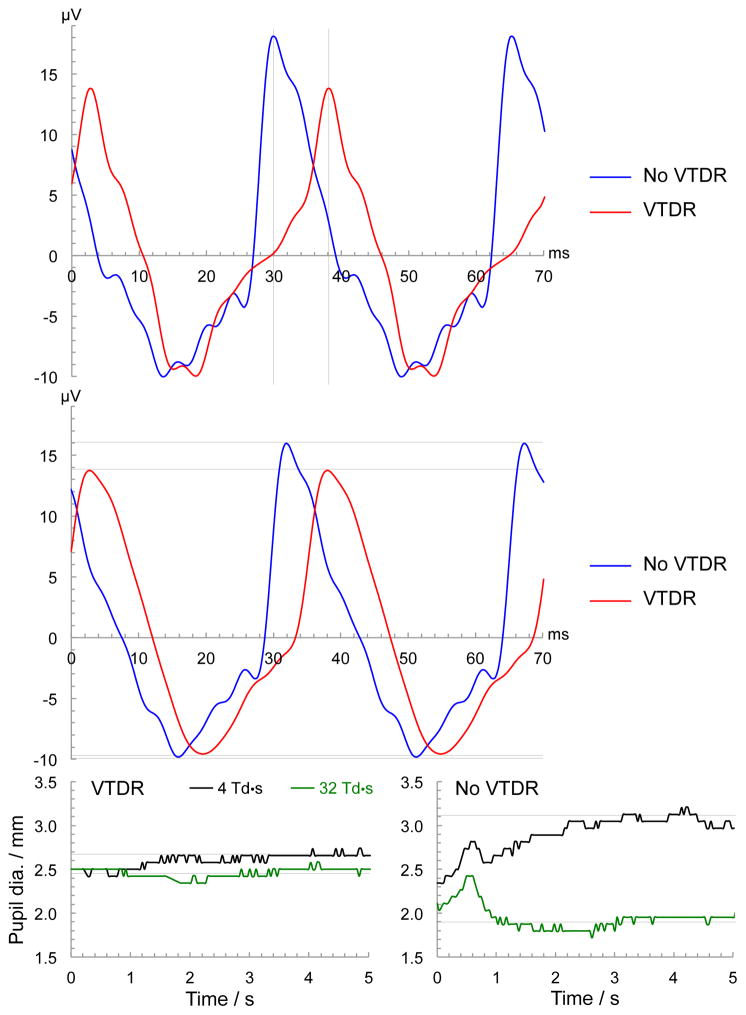
Aims: To evaluate the performance of the RETeval device, a handheld instrument using flicker electroretinography (ERG) and pupillography on undilated subjects with diabetes, to detect vision-threatening diabetic retinopathy (VTDR).
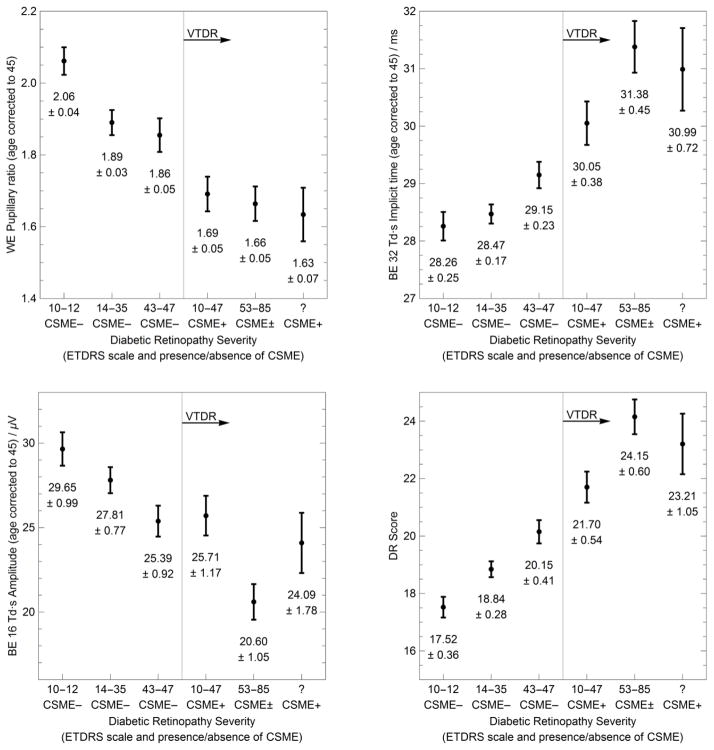
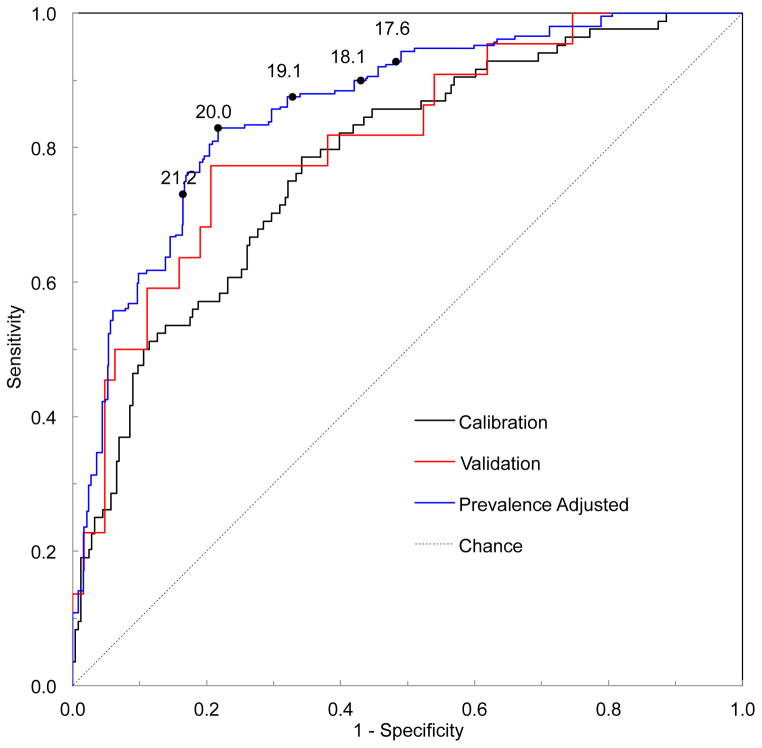
Methods: Performance was measured using a cross-sectional, single armed, non-interventional, multi-site study with Early Treatment Diabetic Retinopathy Study 7-standard field, stereo, color fundus photography as the gold standard. The 468 subjects were randomized to a calibration phase (80%), whose ERG and pupillary waveforms were used to formulate an equation correlating with the presence of VTDR, and a validation phase (20%), used to independently validate that equation. The primary outcome was the prevalence-corrected area under the receiver operating characteristic (ROC) curve for the detection of VTDR.
Results: The area under the ROC curve was 0.86 for VTDR. With a sensitivity of 83%, the specificity was 78% and the negative predictive value was 99%. The average testing time was 2.3 min.
Conclusions: With a VTDR prevalence similar to that in the U.S., the RETeval device will identify about 75% of the population as not having VTDR with 99% accuracy. The device is simple to use, does not require pupil dilation, and has a short testing time.
Keywords: Diabetic eye exam; Diabetic macular edema; Diabetic retinopathy; ERG; Pupillography; Retinal diagnostic test.
Copyright © 2016 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
These conflicts of interest are relevant to this research: grant funding (A.Y. Maa, W.J. Feuer, E.K. Pillow, S.R. Fransen); employment (C.Q. Davis); stock ownership (C.Q. Davis, S.R. Fransen). The remaining authors report no conflict of interest (T.D. Brown, R.M. Caywood, J.E. Chasan).
Figures
References
-
- Centers for Disease Control and Prevention; US Department of Health and Human Services, Centers for Disease Control and Prevention, editor. National Diabetes Fact Sheet, 2011. 2011.
-
- American Academy of Ophthalmology Retina/Viterous Panel; American Academy of Ophthalmology, editor. Diabetic Retinopathy. San Francisco, CA: 2014. Preferred Practice Guidelines.
-
- Paz SH, Varma R, Klein R, Wu J, Azen SP Los Angeles Latino Eye Study G. Noncompliance with vision care guidelines in Latinos with type 2 diabetes mellitus: the Los Angeles Latino Eye Study. Ophthalmology. 2006;113:1372–1377. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
