

Voluntary Cough Airflow Differentiates Safe Versus Unsafe Swallowing in Amyotrophic Lateral Sclerosis
- PMID: 26803772
- PMCID: PMC4871758
- DOI: 10.1007/s00455-015-9687-1
Voluntary Cough Airflow Differentiates Safe Versus Unsafe Swallowing in Amyotrophic Lateral Sclerosis
Abstract
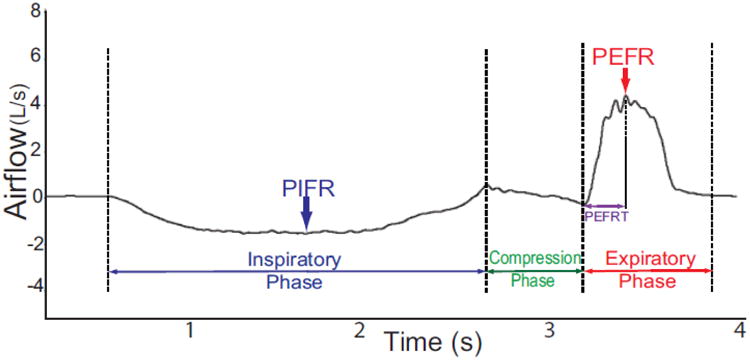
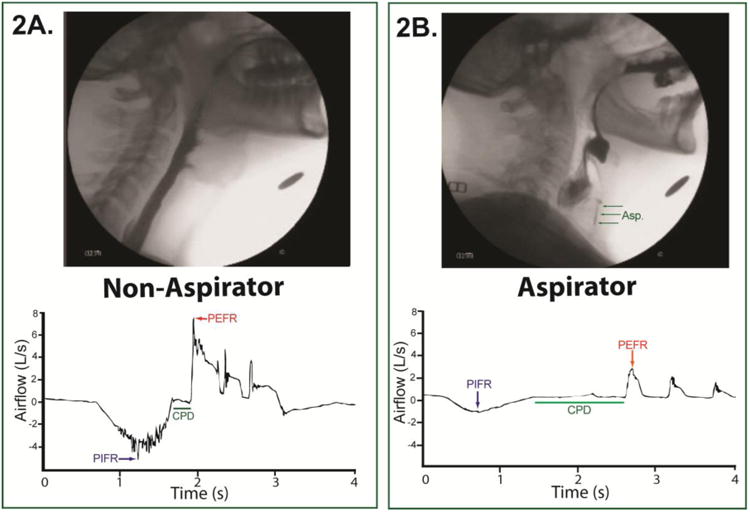
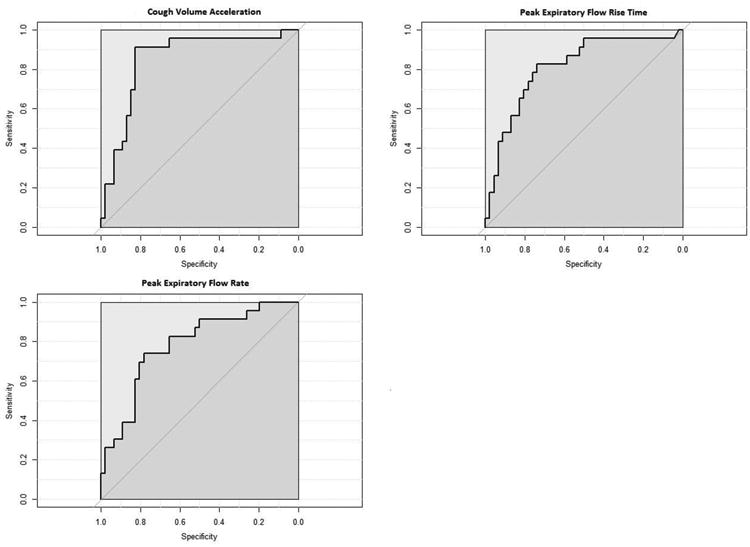
Dysphagia and aspiration are prevalent in amyotrophic lateral sclerosis (ALS) and contribute to malnutrition, aspiration pneumonia, and death. Early detection of at risk individuals is critical to ensure maintenance of safe oral intake and optimal pulmonary function. We therefore aimed to determine the discriminant ability of voluntary cough airflow measures in detecting penetration/aspiration status in ALS patients. Seventy individuals with ALS (El-Escorial criteria) completed voluntary cough spirometry testing and underwent a standardized videofluoroscopic swallowing evaluation (VFSE). A rater blinded to aspiration status derived six objective measures of voluntary cough airflow and evaluated airway safety using the penetration-aspiration scale (PAS). A between groups ANOVA (safe vs. unsafe swallowers) was conducted and sensitivity, specificity, area under the curve (AUC) and likelihood ratios were calculated. VFSE analysis revealed 24 penetrator/aspirators (PAS ≥3) and 46 non-penetrator/aspirators (PAS ≤2). Cough volume acceleration (CVA), peak expiratory flow rise time (PEFRT), and peak expiratory flow rate (PEFR) were significantly different between airway safety groups (p < 0.05) and demonstrated significant discriminant ability to detect the presence of penetration/aspiration with AUC values of: 0.85, 0.81, and 0.78, respectively. CVA <45.28 L/s/s, PEFR <3.97 L/s, and PEFRT >76 ms had sensitivities of 91.3, 82.6, and 73.9 %, respectively, and specificities of 82.2, 73.9, and 78.3 % for identifying ALS penetrator/aspirators. Voluntary cough airflow measures identified ALS patients at risk for penetration/aspiration and may be a valuable screening tool with high clinical utility.
Keywords: Amyotrophic lateral sclerosis; Aspiration; Cough; Deglutition; Deglutition disorders; Screen.
Conflict of interest statement
Authors' Conflict of Interest: None.
Figures
References
-
- Chen A, Garrett CG. Otolaryngologic presentations of amyotrophic lateralsclerosis. Otolaryngol Head Neck Surg. 2005;132(3):500–504. doi:S0194599804018753[pii]10.1016/j.otohns.2004.09.092. - PubMed
-
- Kuhnlein P, Gdynia HJ, Sperfeld AD, Lindner-Pfleghar B, Ludolph AC, Prosiegel M, Riecker A. Diagnosis and treatment of bulbar symptoms in amyotrophic lateral sclerosis. Nat Clin Pract Neurol. 2008;4(7):366–374. doi:ncpneuro0853[pii]10.1038/ncpneuro0853. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
