

Nephrologist-Facilitated Advance Care Planning for Hemodialysis Patients: A Quality Improvement Project
- PMID: 26806003
- PMCID: PMC4921274
- DOI: 10.1053/j.ajkd.2015.11.024
Nephrologist-Facilitated Advance Care Planning for Hemodialysis Patients: A Quality Improvement Project
Erratum in
-
Erratum Regarding "Nephrologist-Facilitated Advance Care Planning for Hemodialysis Patients: A Quality Improvement Project" (Am J Kidney Dis. 2016;68[1]:103-109).Am J Kidney Dis. 2017 Jan;69(1):162. doi: 10.1053/j.ajkd.2016.10.016. Am J Kidney Dis. 2017. PMID: 28007189 No abstract available.
Abstract
Background: The Renal Physicians Association's clinical practice guideline recommends that physicians address advance care planning with dialysis patients. However, data are lacking about how best to implement this recommendation.
Study design: Quality improvement project.
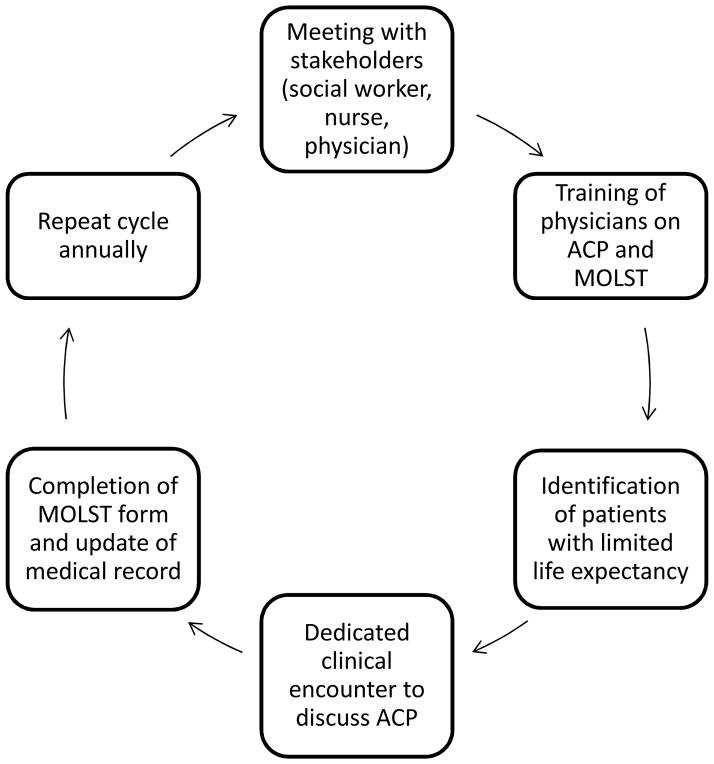
Settings & participants: Nephrologists caring for patients treated with maintenance hemodialysis at 2 dialysis facilities identified patients who might benefit most from advance care planning using the "surprise" question ("Would I be surprised if this patient died in the next year?").
Quality improvement plan: Patients identified with a "no" response to the surprise question were invited to participate in nephrologist-facilitated advance care planning, including completion of a Medical Orders for Life-Sustaining Treatment (MOLST) form.
Outcomes: Change in MOLST completion rate and identification of preferences for limits on life-sustaining treatment.
Measurements: Pre- and postintervention code status, MOLST completion rate, and vital status at 1 year.
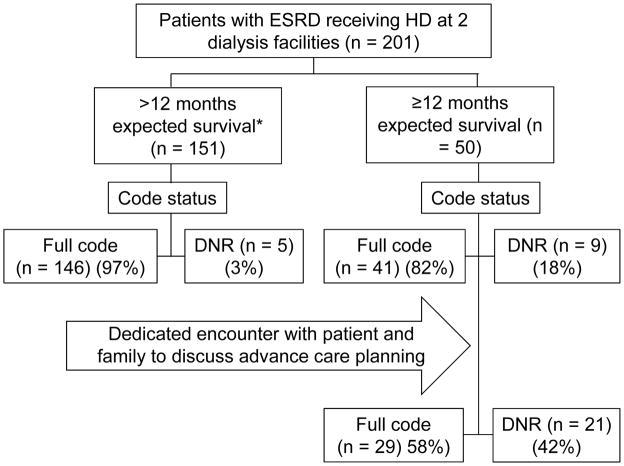
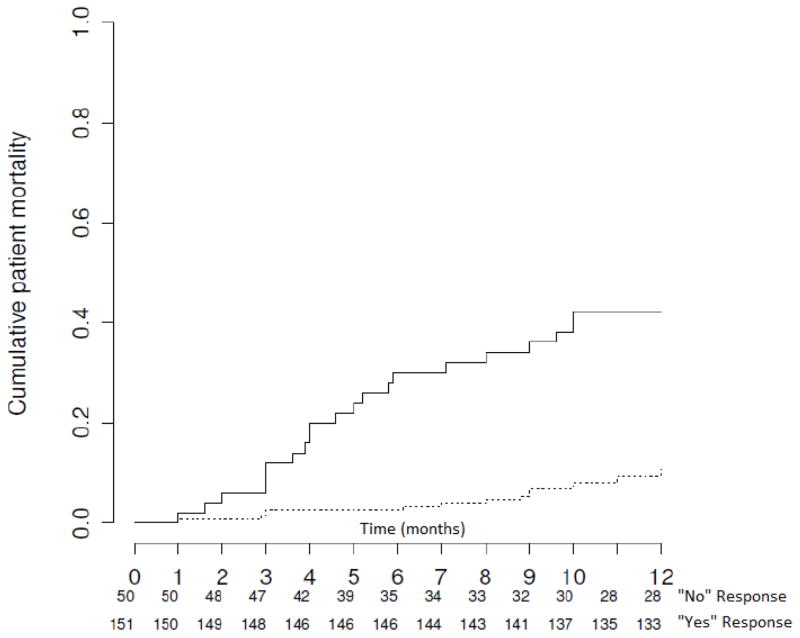
Results: Nephrologists answered "no" to the surprise question for 50 of 201 (25%) hemodialysis patients. Of these, 41 (82%) patients had a full-code status and 9 (18%) had a do-not-resuscitate (DNR) status. Encounters lasted 15 to 60 minutes. Following the encounter, 21 (42%) patients expressed preference for a DNR status and 29 (58%) maintained full-code status (P=0.001). The MOLST completion rate increased from 10% to 90%. One-year survival for patients whose nephrologists answered "no" to the surprise question was 58% compared to 92% for those with a "yes" answer (P<0.001).
Limitations: Sample size and possible nonrepresentative dialysis population.
Conclusions: Nephrologist-facilitated advance care planning targeting hemodialysis patients with limited life expectancy led to significant changes in documented patient preferences for cardiopulmonary resuscitation and limits on life-sustaining treatment. These changes demonstrate the benefit of advance care planning with dialysis patients and likely reflect better understanding of end-of-life treatment options.
Keywords: Advance care planning; cardiopulmonary resuscitation; code status; do not resuscitate (DNR); end-of-life care; end-stage renal disease (ESRD); hemodialysis; life expectancy; medical orders for life-sustaining treatment (MOLST); physician orders for life-sustaining treatment (POLST); quality improvement; shared decision making.
Copyright © 2016 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Planning Dialysis Care: You Might Be "Surprised".Am J Kidney Dis. 2016 Jul;68(1):8-10. doi: 10.1053/j.ajkd.2016.03.002. Am J Kidney Dis. 2016. PMID: 27343808 No abstract available.
References
-
- United States Renal Data System. 2014 Annual Data Report: Epidemiology of Kidney Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda, MD: 2014.
-
- Davison SN, Levin A, Moss AH, et al. Executive summary of the KDIGO Controversies Conference on Supportive Care in Chronic Kidney Disease: developing a roadmap to improving quality care. Kidney Int. 2015;88(3):447–59. - PubMed
-
- Perry E, Swartz R, Smith-Wheelock L, Westbrook J, Buck C. Why is it difficult for staff to discuss advance directives with chronic dialysis patients? Journal of the American Society of Nephrology : J Am Soc Nephrol. 1996;7(10):2160–8. - PubMed
-
- Holley JL, Stackiewicz L, Dacko C, Rault R. Factors influencing dialysis patients’ completion of advance directives. Am J Kidney Dis. 1997;30(3):356–60. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
