

Risk factors and clinical outcomes of arrhythmias in the medical intensive care unit
- PMID: 26807261
- PMCID: PMC4724077
- DOI: 10.1186/s40560-016-0131-x
Risk factors and clinical outcomes of arrhythmias in the medical intensive care unit
Abstract
Background: The clinical impact of arrhythmias on the continuum of critical illness is unclear, and data in medical intensive care units (ICU) is lacking. In this study, we distinguish between different types of arrhythmias and evaluate if their distinction is of clinical importance based on ICU length of stay and mortality outcomes.
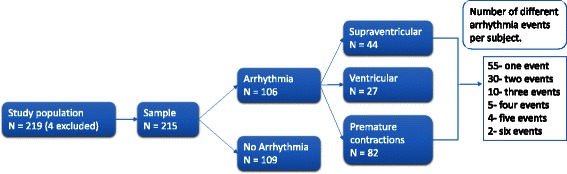
Methods: We performed a retrospective analysis of 215 patients in a community-based teaching hospital medical ICU. Variables gathered include sociodemographic data, arrhythmias identified and interpreted by the study team, and admission diagnoses coded into clinical mediator categories based on theorized common risk pathways. Univariable and multivariable Poisson regression models were used to identify risk factors for developing arrhythmias by type, prolonged length of stay, and hospital mortality.
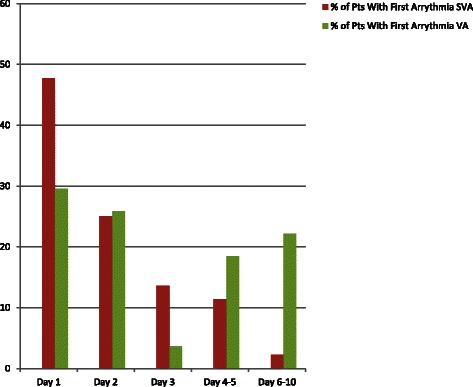
Results: Significant arrhythmia was detected in 28.8 % of subjects with most new arrhythmia events developing within the first 3 days of ICU stay. Acute myocardial ischemia and acute kidney injury at the time of ICU admission were associated with an increased risk of developing supraventricular arrhythmias (SVA) (RR = 2.02; 95 % CI 1.08-3.78 and RR = 1.93; 95 %CI 1.09-3.37, respectively). SVA in the first 3 days of ICU stay was associated with an increased risk of prolonged ICU stay (RR = 1.47; 95 % CI 1.09-1.97). After controlling for clinical mediators, development of SVA was not independently associated with in-hospital mortality. No mediators significantly increased the risk of developing ventricular arrhythmias (VA). VA were not associated to prolonged ICU stay but were associated with increased risk of hospital mortality (RR = 1.93; 95 % CI 1.18-3.15).
Conclusions: It is important to distinguish between supraventricular and ventricular arrhythmias for outcomes in the medical ICU setting. Developing a new VA increases the risk of in-hospital mortality independently. Developing a new SVA increases the risk of having a prolonged ICU stay but does not appear to increase in-hospital mortality independently. These findings suggest that the development of a VA should be considered an independent morbid event and not necessarily the end result of a complicated clinical course, while a new SVA may be considered a cardiac complication of the disease continuum which may add complexity to an ICU stay.
Figures
References
-
- Wong DT, Cheng D, Kustra R, Tibshirani R, Karski J, Carroll-Munro J, et al. Risk factors of delayed extubation, prolonged length of stay in the intensive care unit, and mortality in patients undergoing coronary artery bypass graft with fast-track cardiac anesthesia. Anesthesiology. 1999;91:936–44. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
