

Patient and System-Related Delays of Emergency Medical Services Use in Acute ST-Elevation Myocardial Infarction: Results from the Third Gulf Registry of Acute Coronary Events (Gulf RACE-3Ps)
- PMID: 26807577
- PMCID: PMC4726591
- DOI: 10.1371/journal.pone.0147385
Patient and System-Related Delays of Emergency Medical Services Use in Acute ST-Elevation Myocardial Infarction: Results from the Third Gulf Registry of Acute Coronary Events (Gulf RACE-3Ps)
Abstract
Background: Little is known about Emergency Medical Services (EMS) use and pre-hospital triage of patients with acute ST-elevation myocardial infarction (STEMI) in Arabian Gulf countries.
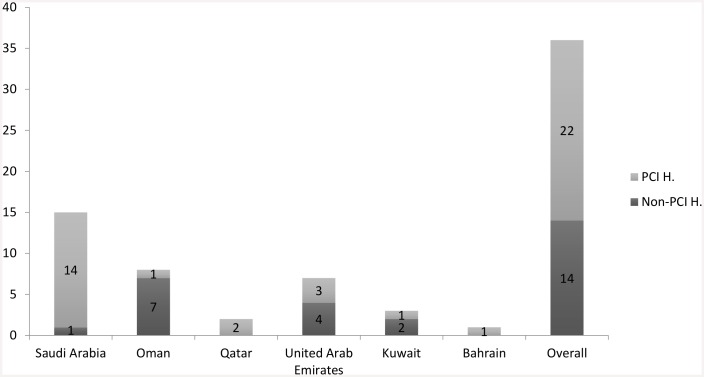
Methods: Clinical arrival and acute care within 24 h of STEMI symptom onset were compared between patients transferred by EMS (Red Crescent and Inter-Hospital) and those transferred by non-EMS means. Data were retrieved from a prospective registry of 36 hospitals in 6 Arabian Gulf countries, from January 2014 to January 2015.
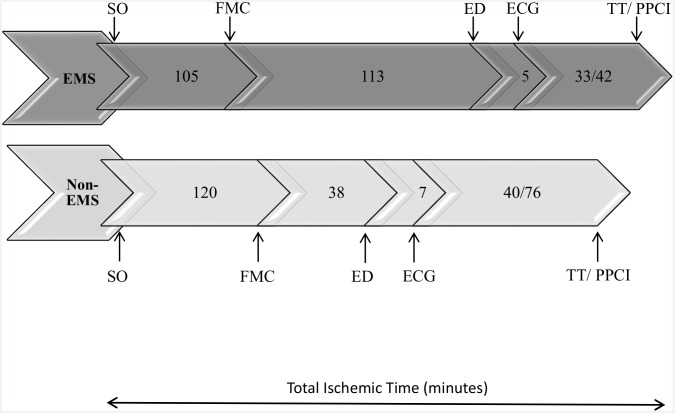
Results: We enrolled 2,928 patients; mean age, 52.7 (SD ±11.8) years; 90% men; and 61.7% non-Arabian Gulf citizens. Only 753 patients (25.7%) used EMS; which was mostly via Inter-Hospital EMS (22%) rather than direct transfer from the scene to the hospital by the Red Crescent (3.7%). Compared to the non-EMS group, the EMS group was more likely to arrive initially at a primary or secondary health care facility; thus, they had longer median symptom-onset-to-emergency department arrival times (218 vs. 158 min; p˂.001); they were more likely to receive primary percutaneous coronary interventions (62% vs. 40.5%, p = 0.02); they had shorter door-to-needle times (38 vs. 42 min; p = .04); and shorter door-to-balloon times (47 vs. 83 min; p˂.001). High EMS use was independently predicted mostly by primary/secondary school educational levels and low or moderate socioeconomic status. Low EMS use was predicted by a history of angina and history of percutaneous coronary intervention. The groups had similar in-hospital deaths and outcomes.
Conclusion: Most acute STEMI patients in the Arabian Gulf region did not use EMS services. Improving Red Crescent infrastructure, establishing integrated STEMI networks, and launching educational public campaigns are top health care system priorities.
Conflict of interest statement
Figures

References
-
- O’Gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, et al. ; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/ American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:e362–e425. 10.1161/CIR.0b013e3182742cf6 - DOI - PubMed
-
- Kristensen SD, Laut KG, Fajadet J, Kaifoszova Z, Kala P, Di Mario C, et al. ; European Association for Percutaneous Cardiovascular Interventions. Reperfusion therapy for ST elevation acute myocardial infarction 2010/2011: current status in 37 ESC countries. Eur Heart J. 2014; 35:1957–70. 10.1093/eurheartj/eht529 - DOI - PubMed
-
- Jacobs AK, Antman EM, Ellrodt G, Faxon DP, Gregory T, Mensah GA, et al. ; American Heart Association's Acute Myocardial Infarction Advisory Working Group. Recommendation to develop strategies to increase the number of ST-segment-elevation myocardial infarction patients with timely access to primary percutaneous coronary intervention. Circulation 2006;113:2152–2163. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
